
More Information
Submitted: November 11, 2019 | Approved: March 16, 2022 | Published: March 17, 2022
How to cite this article: Woodman R. The examination and treatment of non-surgical soft tissue injuries at the elbow integrating the Cyriax approach with the mulligan concept. J Sports Med Ther. 2022; 7: 001-005.
DOI: 10.29328/journal.jsmt.1001054
Copyright License: © 2022 Woodman R. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

The examination and treatment of non-surgical soft tissue injuries at the elbow integrating the Cyriax approach with the mulligan concept
Russell Woodman*
Professor Emeritus, Quinnipiac University, Hamden, USA
*Address for Correspondence: Russell Woodman, PT MS DPT OCS MCTA FSOM, Professor Emeritus, Quinnipiac University, Hamden, USA, Email: russell.woodman@quinnipiac.edu
Injuries at the elbow are fairly common. Fractures require the immediate attention of the skills of a surgeon. As the fracture heals and motion at the fracture is permissible, the physical therapist can provide important treatment to help the patient gain range of motion, strength, and function.
Non-surgical problems at the elbow include sprained ligaments, tendinopathies, bursitis, nerve injuries, loose bodies, and capsulitis. Tennis players are vulnerable to lateral epicondylitis if their form on the backhand stroke is incorrect. Bowlers may experience medial elbow pain due to overuse of their wrist flexors and/or pronators. Excessive and painful valgus stress is frequently experienced by baseball pitchers.
The purpose of this article is to introduce the integration of the examination and treatment approach developed by Dr. James Cyriax with the Mulligan concept of physical therapy for treating painful loss of elbow joint range of motion and tendinopathies [1].
Cyriax examination of the elbow
The examining clinician must keep in mind that lesions at the cervical spine and/or shoulder can refer to pain to the elbow. This is particularly true if the patient’s complaints start proximal to the elbow.
Therefore at the clinician’s discretion, it may be necessary to perform an examination of the cervical spine and shoulder before examining the elbow.
History
When taking a history for soft tissue lesions at the elbow, the following are examples of what may have occurred:
1. The patient may have experienced a sudden loss of either elbow flexion or extension. The onset can be secondary to an event or maybe insidious. The loss of range of motion may be due to a loose body in the elbow or a positional fault limiting motion in one direction.
2. The patient may have a loss of both elbow flexion and extension. This may be secondary to an arthritic condition. Typically, at the elbow when arthritis occurs, the loss of flexion is greater than the loss of extension. Traumatic arthritis may occur after a fall on the elbow. With trauma, the loss of range of motion occurs almost immediately. Osteoarthritis and rheumatoid arthritis tend to have a more gradual onset.
3. Tendinopathies usually have a gradual onset of pain associated with muscle overuse. Although sometimes the patient will report a sudden onset. Strong and painful muscle testing is consistent with tendinopathy. Severe tendinopathy will elicit a weak painful response.
4. Typically, muscle belly strains frequently have a sudden onset. A grade one strain will exhibit a strong and painful response on muscle testing. A grade two or three strain will elicit a weak and painful response.
5. The patient may have developed elbow pain secondary to a sports injury such as poor body mechanics on a backhand stroke in tennis.
The examiner should consider ultrasound or MRI imaging when muscle testing elicits a weak and painful response. The imaging can rule in or out a partial tear in the contractile tissue. Furthermore, the examiner should consider a radiograph to rule out a possible fracture at the muscle’s bony attachment.
Inspection
History documentation is followed by an inspection. Severe muscle strains will cause localize subdermal bleeding (Figure 1). Olecranon bursitis is very visible on the posterior aspect of the elbow (Figure 2).

Figure 1: Subdermal Bleeding.

Figure 2: Olecranon Bursitis.
Selective tissue tension testing
A variety of tests are documented in the literature. Most soft tissue lesions can be diagnosed by performing ten selective tissue tension tests. When performing passive tests, the examiner is assessing a range of motion, end feel, and potential reproduction of pain. At the elbow the normal end feel for flexion is tissue approximation, extension is boney, supination and pronation are capsular.
When performing mid-range isometric muscle testing consider the following:
a) Strong and Painless (SPL) = Muscle is normal
b) Strong and Painful (SPF) = Minor tendinopathy or minor muscle strain
c) Weak and Painless (WPL) = Peripheral nerve lesion or Total tear of the muscle
d) Weak and Painful (WPF) = Severe tendinopathy or severe muscle strain, or fracture
Table 1 is a useful evaluation form.
| Table 1: Useful evaluation form. | ||||
| Elbow Evaluation Form | ||||
| History | ||||
| Inspection | ||||
| Selective Tissue Tension | ||||
| Passive | Pain | End Feel | ROM | |
| Flexion | ||||
| Extension | ||||
| Supination | ||||
| Pronation | ||||
| Resistive | SPL | SPF | WPL | WPF |
| Elbow Flexion | ||||
| Elbow Extension | ||||
| Elbow Supination | ||||
| Elbow Pronation | ||||
| Wrist Flexion | ||||
| Wrist Extension | ||||
Valgus stress test is an accessory test for a sprained ulnar collateral ligament and compression of the radial head. It is illustrated in Figure 3.

Figure 3: Valgus testing at the elbow.
The following serves as an introduction on how to employ the Cyriax algorithm to reach a diagnosis.
The examiner must make a judgment as to which selective tissue tension tests are most painful. The passive or the resisted and then combine that information with history and inspection to reach a diagnosis.
If the passive motions are more painful the examiner must decide if the patient is in the capsular pattern of arthritis or is in the non-capsular pattern. The capsular pattern at the elbow is indicative of arthritis. The capsular pattern is a greater loss of flexion than extension. Only in long-standing arthritis will pronation and supination become limited.
A common cause of a loss of elbow motion in the non-capsular pattern is a loose body within the joint. In this situation, most typically, either flexion or extension exhibit a small loss of motion, sometimes pronation or supination will also have a small loss of motion.
If the resisted motion is more painful, then the lesion lies within the muscle belly (strain) or its boney attachment (tendinopathy). Lesions can occur in any of the muscles that span the elbow joint. Since the wrist flexors and extensors originate on the humerus, muscle testing of wrist flexion and extension is part of the elbow exam. Some of Mulligan’s greatest contribution includes mobilization with movement for tennis elbow (painful wrist extension) and golfer’s elbow (painful wrist flexion) [2].
Examples of soft tissue problems at the elbow and physical therapy
Traumatic arthritis of the elbow: Traumatic arthritis can occur in any age group. This may occur as a result of a falling injury.
After about 24 hours, the patient develops a painful loss range of motion. The joint capsule is inflamed and the patient is in the capsular pattern of arthritis. The clinician must keep in mind that if passive pronation and/or supination are also painful that the radial head is fractured. If any question exists, a radiograph must be obtained.
Unlike traumatic arthritis of the shoulder, the patient with traumatic arthritis at the elbow can’t receive stretching into flexion and extension within the first 3-4 weeks of injury. This is because of the possible presence of bleeding into the brachialis muscle belly which can occur along with the trauma to the elbow’s capsule. The red blood cells have the potential to become bone cells through a process known as metaplasia. The development of these bone cells causes myositis ossificans (Figure 4). If myositis ossificans bridge the elbow joint the patient will lose range of motion.
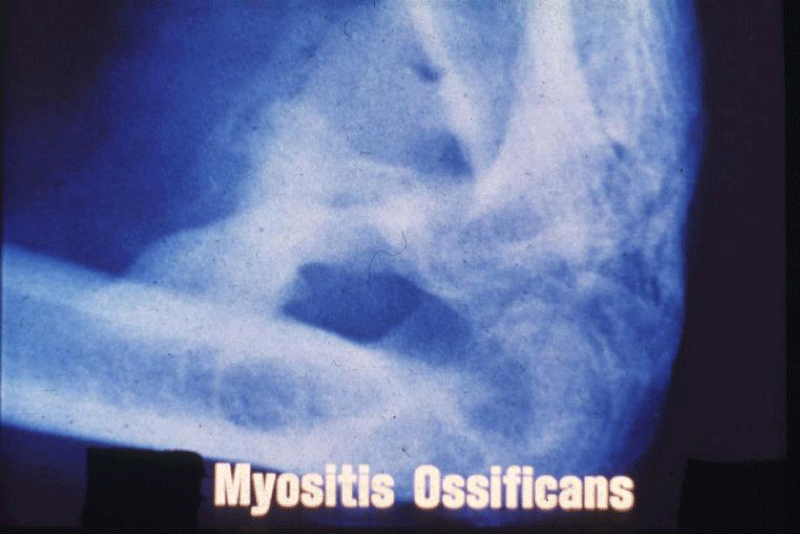
Figure 4: Myositis Ossificans.
Aggressive stretching with the first 3-4 weeks of therapy, can cause more bleeding and the potential for a greater amount of myositis ossificans.
It is therefore recommended, during the early stage, that the patient either rest their arm in a sling or receive a steroid elbow joint injection to alleviate the inflammation. More information about this is available in Ombregt’s book System of Orthopaedic Medicine [3].
Once the four-week period has passed, it is not likely that the passive range of motion will cause an increase of bleeding into the brachialis. A joint mobilization technique such as flexion and extension mobilization with movement can now be an effective and safe way of improving in a pain-free manner elbow flexion and extension
A review of the literature identified two case study articles advocating exercise within the first month of elbow traumatic arthritis De Carlo’s article on the rehabilitation of the patient with myositis ossificans offers a gentle joint mobilization approach to improve elbow motion [4]. Ebaugh and Gard treated a 19-year-old hockey player with a severe elbow flexor contusion which they believed was developing myositis ossificans [5]. They found that a combination of one treatment pulsed ultrasound, 9 treatments acetic acidiontophoresis, and gentle elbow range of motion exercises were successful as the patient gained normal pain-free elbow range of motion.
Loose Body in the Elbow Joint-This may be secondary to trauma, but frequently, the onset is insidious. The patient states that they suddenly developed a loss of either flexion or extension at the elbow. On passive joint testing, the clinician will probably elicit a springy end feel on either flexion or extension with a 10-15-degree loss of motion. Sometimes the loose body also blocks pronation or supination. It depends on precisely where the loose body is within the joint. Figure 5 is a sagittal CT scan of an interesting and unusual situation where loose bodies are located both anteriorly and posteriorly. It is likely that in this case both flexion and extension would be limited. This would present a challenge. This CT scan was selected for this article to illustrate potential locations for a loose body.

Figure 5: Loose bodies in the elbow.
We must keep in mind that unless imaging was performed, the loose body remains a clinical diagnosis based on history and physical exam.
Cyriax’s manipulation is very effective to move the loose body within the joint to a pain-free location, however, it requires three clinicians to administer it (Figure 6) Mulligan’s mobilization with movement only requires one clinician and a mobilization belt (Figure 7). Frequently, the patient only requires 1-3 sessions of therapy to maintain indefinitely the loose body in a pain-free location. The patient must be informed that sometime in the future the joint blockage may re-occur, and they will once again require therapy. If the loose body has occurred in a youngster who has not fully grown, it is recommended that the loose body is removed surgically. This is because as the child grows, the synovial fluid within the elbow joint will provide nourishment to the loose body and it will grow and more severely block elbow motion.

Figure 6: Manipulation for a loose body at the elbow.

Figure 7: Mobilization with the movement for a loose body at the elbow.
Positional fault at the elbow joint: An important hypothesis that provides an explanation for the improvement gained utilizing mobilization with movement is the “positional fault hypothesis”. Both Sahrmann and McConnel both propose that faulty position of bones can have an adverse effect on joint range of motion. For example, Sahrmann describes how excessive humeral internal rotation during shoulder flexion can result in limited and painful shoulder motion. Cook supports Sahrmann’s hypothesis, pointing out that shoulder impingement is more likely if the shoulder lacks adequate humeral external rotation during shoulder elevation [6].
McConnel states that the faulty position of the patella within the trochlear notch leads to patellofemoral pain. Allen’s [7] MRI study of patients with anterior knee pain supports McConnel’s hypothesis, as he points out that there is a direct correlation between anterior knee pain and incorrect tracking of the patella.
As related to Mulligan’s mobilization with movement Hing and his colleagues in the book “Mobilisation with Movement” have written an excellent chapter on the positional fault hypothesis [8]. A few of the key points that summarize this chapter are:
a) The positional fault hypothesis proposes that mobilization with movement corrects minor bony incongruities
b) There is evidence that positional faults may occur in the inferior tibiofibular, patellofemoral, and shoulder joints
c) There is little research into the effects of mobilization with movement on positional faults
Here is an interesting diagnostic challenge. When examining a patient with a sudden painful loss of elbow range of motion such as a loss of flexion, extension, and/or pronation is supination how would we know if the patient has a positional fault or a loose body in the joint? Is the end feel springy? Is it a loose body or a positional fault?
Hing points out that measurements of positional faults are achieved largely through imaging techniques that are not readily available to the practitioner of MWM [9].
Loose bodies with an osseous component are visible on radiograph and those of pure cartilage is most likely to be seen on CT scan. However, in many instances, imaging is not available to the physical therapist. Furthermore, it would be time-consuming and expensive to send such a patient for imaging to confirm the diagnosis. Most therapists would agree that it is better to perform joint mobilization and see if the patient can be improved. Figure 8 illustrates one example of mobilization with movement for a “positional fault” at the elbow for a loss of elbow extension. In Figure 8, the therapist is performing medial glide of the ulna combined with active elbow extension and passive overpressure at end range by the therapist. Sometimes lateral glide of the ulna works best, sometimes the ulna must be internally or externally rotated.

Figure 8: Medial glide of the olecranon.
Tennis elbow and golfers elbow: These two conditions are relatively easy to identify. Tennis elbow, tendinopathy of the extensor mechanism causes lateral elbow pain. Isometric wrist extension is strong and painful. Golfers elbow, tendinopathy of the flexion mechanism causes medial elbow pain. Isometric wrist flexion is strong and painful. Cyriax did a masterful job in identifying the specific locations of each of these lesions. Certain locations respond to deep friction massage. Other locations are improved rapidly with a steroid injection or anesthetic injection.
Figure 9 illustrates the locations for tennis elbow. Ombregt’s text and the earlier textbook by Cyriax, Orthopaedic Medicine are excellent references for more details of the Cyriax approach.
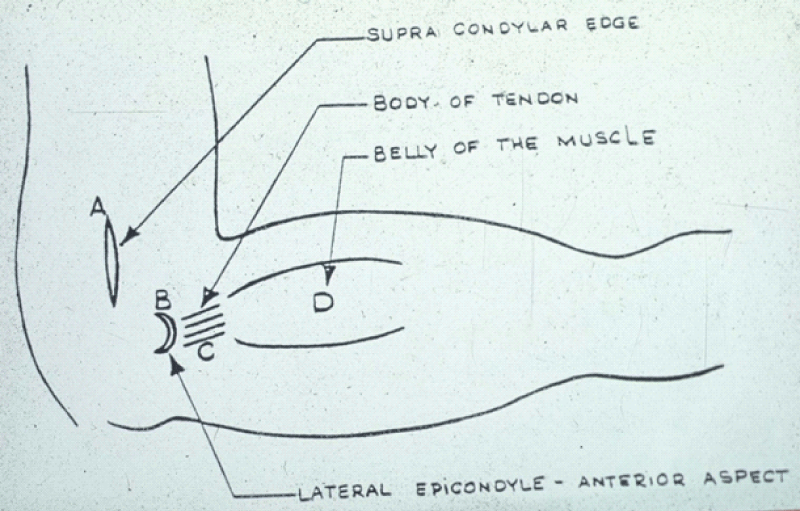
Figure 9: Locations of tennis elbow, Recommendation of treatment for each location. A-Deep Friction Massage; B-Cortisone Injection or Deep Friction Massage followed by Mills manipulation; C-Deep Friction Massage; D- Anesthetic injection or Deep Friction Massage.
It has been this author’s experience that the mobilization with a movement developed by Mulligan is very effective for more than ½ of the patients he has seen. However, when not effective, the Cyriax approach is very valuable for improving the patient.
Concerning tennis elbow, Bisset and Vicenzino [10] state that “The underlying mechanism by which the mobilization with movement produces a rapid change in previously painful motor activity is not fully understood. It is thought to involve the activation of endogenous pain control mechanisms. It has been postulated that the afferent input that is provided by the application of mobilization is sufficient to trigger these innate mechanisms.”
Figure 10 illustrates the initial position for performing mobilization with movement for tennis elbow.

Figure 10: Mobilization with the movement for tennis elbow.
At least 9 research articles have been published on mobilization with movement for tennis elbow. Bisset compared the effectiveness of mobilization with movement for tennis elbow and exercise compared to a wait and see approach or cortisone injection. Mobilization with movement and exercise was superior for reducing pain to both a wait-and-see approach and cortisone injection. Bagadev’s [11] study supports Bisset’s study [8]. Patients had lower DASH and VAS scores when mobilization with movement was compared to steroid injection at a follow time of 24 weeks after completion of treatment. Moon’s research demonstrated that mobilization with movement performed every other day for ten days was superior to a placebo group [12].
The program in the clinic should be combined with a mobilization home program to be done daily in order to get long-lasting pain relief. Figure 11 illustrates the starting position for the home program.

Figure 11: Starting position for the home program for tennis elbow.
Figure 8 illustrates the medial glide of the ulna is in the same position the patient is placed in for MWM for the golfer’s elbow. The difference is that instead of asking the patient to extend their elbow, the patient is instructed to perform wrist flexion. This can be done by telling the patient to squeeze the therapist’s left elbow or perform wrist flexion with a lightweight. Remember that will all MWMS, if indicated, the provocative motion is now pain-free.
The Cyriax approach for Golfers’s elbow is less complex compared to the tennis elbow [1]. Golfers’ elbow at the medial condyle of the forearm flexors is responded more rapidly to a cortisone injection than deep friction massage, and the musculotendinous junction will only respond to deep friction massage.
- Cyriax J. Textbook of Orthopaedic Medicine Vol 1 Diagnosis of Soft Tissue Lesions 6th ed. Bailliere Tindal London. 1976.
- Mulligan B. Manual Therapy “NAGS”, “SNAGS”, “MWMS” etc. distributed by OPTP, Minneapolis, Minnesota.
- Ombregt L. A System of Orthopaedic Medicine Churchill Livingstone 3nd ed. Elsevier Australia. 2013.
- De Carlo M. Rehabilitation of myositis ossificans in the brachialis muscle. J Athl Train. 1992; 27: 76-79. PubMed: https://pubmed.ncbi.nlm.nih.gov/16558137/
- Ebaugh D, Gard K. The use of acetic acid iontophoresis in the management of a soft tissue injury. N Am J Sports Phys Ther. 2010; 5: 220-226. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096143/
- Cook T, Ludewig P. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phy Ther. 2000; 8: 276-291. PubMed: https://pubmed.ncbi.nlm.nih.gov/10696154/
- Allen G. Significant association between anterior knee pain and abnormal tracking. Skeletal Radiol. 1999 28: 220-223.
- Hing W. Mobilisation with Movement-The art and the science Elsevier Australia 2011
Marga M. The epidemiology of injuries to the elbow in sport. Int Sports Med.J. 2005; 6: 25-33. - Hing W, Hall T, Mulligan B. The Mulligan Concept of manual therapy. Elsevier Australia. 2015.
- Bisset L, Beller E, Jull G, Brooks P, Darnell R, et al. Mobilization with movement and exercise compared to corticosteroid injection or wait and see for tennis elbow: A randomized trial. BMJ. PubMed: https://pubmed.ncbi.nlm.nih.gov/17012266/
- Bagade V. Mobilization with the movement for treatment of chronic lateral epicondylitis: 24 weeks follow up. Ind J Physiother Occupational Ther. 2015; 9: 200-2003.
- Moon D. Improvement of pain and functional activities in patients with lateral epicondylitis by MWM; A random placebo controlled study. J Phy Ther Sci. 2012; 24: 787-790.