
More Information
Submitted: 18 December 2019 | Approved: 23 December 2019 | Published: 24 December 2019
How to cite this article: Emmanouil S, Iain G, Nikolaos C, Eirini G, Andres A, et al. The effect of a European-based exercise program upon the health-related physical fitness of individuals with intellectual disabilities: The alive and kicking perspective. J Sports Med Ther. 2019; 4: 081-093.
DOI: 10.29328/journal.jsmt.1001048
Copyright License: © 2019 Emmanouil S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

The effect of a European-based exercise program upon the health-related physical fitness of individuals with intellectual disabilities: The alive and kicking perspective
Skordilis Emmanouil1*, Greenlees Iain2, Chrysagis Nikolaos1, Grammatopoulou Eirini1, Arriaga Andres3, Vaquero Fernandez Almudena3, Gaillard Joel4, Skordilis Antonios5, Dias Joao6, Papadopoulou Vassiliki7 and Serras Dionysios7
1National and Kapodistrian University of Athens, School of Physical Education and Sport Science, Greece
2Chichester Institute of Sport, University of Chichester, UK
3Universidad Europea, Madrid, Spain
4Universite de Lorraine, France
5Amfidromo Chorotheatro, Cyprus
6Associacao Para A Recuperacao De Cidadaos in Adaptados De Lousa, Portugal
7Ploes EPSYME, Psychosocial Research Organization, Drapetsona, Piraeus, Greece
*Address for Correspondence: Skordilis Emmanouil, National and Kapodistrian University of Athens, School of Physical Education and Sport Science, Greece, Email: eskord@phed.uoa.gr
The present study examined the effect of the European-Based ‘Alive and Kicking’ exercise program on the health-related physical fitness of individuals with (Experimental Group: EG) and without (Control Group: CG) (Intellectual Disability: ID). The Self-Determination Theory: SDT, guided both the 6-month preparatory phase and the 9-month exercise program, which was conducted in five separate European countries (Cyprus, France, Greece, Portugal and Spain). The total sample (n = 200, 54% males and 46% females) comprised of 168 individuals with ID (age: 26.54 years, + 7.78) and 32 individuals without ID (age: 25.81 years, + 8.73) respectively. The statistical analyses revealed that the ID group’s performance (EG) improved significantly in a range of health-related physical fitness variables (sit & reach, pushups, sit ups, long jump, ½ mile walk/ run). In turn, the participants from the CG improved mainly in muscular endurance (sit ups and pushups). The results are discussed in accordance with SDT and the dairies kept from the staff involved (coaches and psychologists) during the 9–month intervention. The present findings, although subjective to certain limitations, are encouraging, given the large-scale, real-world nature of the research design, and provide evidence supporting the integration of theoretical strategies enhancing motivation into traditional coaching programs for individuals with ID.
Individuals with intellectual disability (ID) experience elevated risks for several health problems associated with physical inactivity [1,2]. The physical inactivity is mainly due to their predominantly sedentary lifestyle [1,3,4] and may lead to increased rates of morbidity and mortality [5]. Common health problems are the increased rates of diabetes, obesity, elevated blood pressure and cholesterol levels, and low physical fitness [6-10].
The physical fitness of individuals with ID has been examined and the research findings consistently indicate that they a) do not meet the general fitness criteria [4,11] and b) are less fit compared to the general population [9,10]. Skowronski, et al. [12], summarized previous research efforts conducted in the United States and in Europe and claimed that a continuing pattern of low fitness for individuals with ID is consistently observed [12]. Additionally, individuals with ID show faster declines in fitness over the life-span, compared to individuals without ID, leading to a wider risk for associated health problems [9].
Stanish, et al. [11], claimed that individuals with ID are usually not included in several population studies documenting exercise and physical activity (PA) campaigns for health promotion. The ‘Pomona’ project described a set of health indicators for individuals with ID, in 13 separate European state members [13]. The researchers claimed that several indicators, leading to a healthy lifestyle, such as diet and exercise, may assist in the shaping of national policies, and the enhancement of quality of life for individuals with ID [13]. The ‘Closing the Gap’ was another initiative in the U.S.A., that outlined the actions required to improve the health disparities, while exercise and fitness were prescribed as main targets to promote health [14].
Stanish, et al. [11], suggested that the absence of health promotion strategies for individuals with ID may be of high concern due to the a) high medical burden (direct cost due to several chronic diseases related to inactivity) and b) lost wages, absenteeism, work limitations, premature death, etc. (indirect cost) [11]. According to Temple, et al. [4], similar costs have been estimated in several industrialized countries [15,16], while Stancliffe, et al. [17], suggested that besides the direct and indirect costs, there are emotional and social consequences from inactivity which are difficult to assess. The social and emotional burdens of inactivity will further restrict their independence, despite their desire to have control of their lives. Stancliffe, et al. [17], concluded that determination to overcome social and emotional barriers and overall social integration in individuals with ID are related to their health which, in turn, is influenced by their motivation to engage in daily activities such as exercise and physical activity (PA) programs.
The self – determination theory (SDT), a general recent motivation theory, guided the present study [18,19]. According to Deci and Ryan, [18], the establishment of certain behaviors and the changing of daily habits require the satisfaction of certain psychological needs. The SDT prescribes autonomy, competence and relatedness as inherent and universal psychological needs affecting directly the individual’s engagement in certain desirable behaviors, such as exercise, diet, dental care etc. [20]. The need for autonomy refers to the feeling of choice and volition act, the need for competence refers to the feeling of being effective in achieving certain desired outcomes and the need for relatedness refers to the feeling of sharing and mutual care [21]. Deci, et al. [22], claimed that these needs are vital for people to flourish, experience wellness and prevent maladaptive behaviors, regardless of their intellectual functioning. By maximizing therefore the individual’s universal psychological needs of autonomy, competence, and relatedness, the upcoming health-related behaviors (e.g. engagement in exercise) will be internalized and sustained [23].
In general, the SDT interventions are designed to assist individuals’ progress on a continuum towards an intrinsic form of motivation, when their inherent psychological needs are satisfied and certain behaviors are driven due to elements such as spontaneity, enjoyment, share and interest [24,25]. Farrell, et al. [24], suggested that intrinsic motivation may be the target for engagement in exercise, unlike other health behaviors such as wearing a seat belt or brushing teeth, ‘by honing in on people’s natural interest and enjoyment in activities such as sports, dancing, water activities’ (p 154) etc. Within the above continuum, when these needs are not fulfilled, the individuals may experience an extrinsic motivation form, from external sources, such as winning medals, competitions, monetary rewards, please of their coaches, teachers and family members etc. [19,26]. At the other end, when engagement is neither intrinsically nor extrinsically rewarded, and the individual has no intention to act and participate, he/she experiences amotivation towards the desired outcome. Amotivation is likely to emerge when the engagement in an activity (e.g. an exercise or a PA program) is not valued, it may not result in desired outcomes, or because it may lead to feelings of incompetence [19].
Researchers have used the SDT as a general framework to design and implement exercise and PA programs for individuals mainly without ID [27-32]. Recently, the research effort shifted towards individuals with ID [33-38] with promising results, albeit limited in scope. Further, the review studies retrieved [4,11,39,40] did not specifically examine the intermediate effect of the SDT interventions towards the engagement in exercise and PA for individuals with ID. Bodde, et al. [33], examined the effect of a health education program and found improvement upon nutritional knowledge and overall involvement in PA in a sample of adults with mild – moderate ID [33]. Johnson, et al. [36], examined the effect of two different autonomy supported climate conditions (high vs. low autonomy), upon the PA involvement of individuals with and without developmental and intellectual disabilities. The researchers found that all participants involved spent increased time in PA during the high autonomy supported climate in class [36]. Di Lorito, et al. [34], developed a 12-month intervention protocol, with an activity behavior change approach assimilating the elements of the SDT, in a sample of patients with early dementia and mild cognitive impairment. The researchers reported that the elements of motivation, autonomy, support and control may mediate the successful effect of the organized program [34]. Kraiss, et al. [37], examined the effect of a 6-week wearable technology program upon the involvement in PA of adults with intellectual and developmental disabilities. The researcher used the SDT principles and recorded a consistent pattern of improved PA levels across time, for all participants involved [37]. Simpson, et al. [38], studied the effect of a twelve – session intervention program, upon the fitness and skill levels of ten adolescents with developmental and physical disabilities. The researcher found a significant improvement and attainment of the participant’s goals [38]. Kelly, et al. [35], examined the effect of a six – week yoga intervention period upon the self – determination elements and the anxiety of adults with developmental and intellectual disabilities. The researcher found that the program was effective and managed to improve self – determination and decrease the anxiety levels of the individuals involved [35].
Taken together, the fulfillment of the universal psychological needs (autonomy, competence and relatedness) and the attainment of intrinsic motivation may lead to the necessary involvement in exercise and PA programs, which, in turn, may guide individuals with ID across their life span [41,42]. The above objective is essential if we consider that these individuals often experience failure in ordinary daily activities, limited feedback of successful social behaviors and adoption of extrinsic motivation and amotivation patterns [43]. The extrinsic means to enhance motivation [44,45] may lead to a decrement of spontaneous activity [46], dependence from sustained external reinforcements [43,47] and less inclination to participate in organized exercise and PA [41]. Pozeriene, et al. [48], however disputed that argument and suggested that individuals with ID are often involved in certain behaviors through extrinsic rewards. These rewards, accompanied with the constant reinforcement from significant others, are important at the initial stages of their participation and may eventually lead to spontaneous activity involvement [48]. The argument of Pozeriene, et al. [48], is strengthened from their involvement in Special Olympics, where they often choose to participate in different sports mainly due to the extrinsic rewards [49], travelling experiences and the influence from their intimate environment and coaches [50]. Finalizing the research findings and despite the above conflict, it appears that the ongoing study of motivation, PA and exercise for individuals with ID may eventually assist ‘our understanding of the psychological processes underlying participation, and assist in designing effective interventions’ [51] in the future.
Based on the above and the limited number of large scale population research, the present study was designed to examine the effect of the ‘Alive and Kicking’ exercise program conducted in five European countries, based on the self-determination theory (SDT), upon the physical fitness of the individuals with intellectual disabilities (ID) involved. Exercise was perceived as ‘a subcategory of physical activity that is planned, structured and organized, undertaken for maintaining or improving fitness’ [52]. Physical fitness, in turn, was defined as ‘a measure of the body’s ability to function efficiently and effectively in work and leisure activities, to be healthy and to resist in hypokinetic diseases’ [53,54]. In the present study, the health-related physical fitness was introduced, consisting ‘of those components of physical fitness that have a relationship with good health. The components are commonly defined as body composition, cardiovascular fitness, flexibility, muscular endurance and strength’ [55]. The independent variables were group (experimental: individuals with ID, and control: individuals without ID) and time (pre, intermediate and post testing). The dependent variables were the health-related physical fitness measures of aerobic capacity, muscular endurance, explosive strength, flexibility, agility and anthropometric measures.
Participants
A total of 200 individuals were involved in the present study (males 54%, females 46%). The total sample was divided in two parts: a) the experimental group (EG) consisting from 168 participants with ID, and b) the control group (CG) consisting from 32 participants without ID. Intellectual disability (ID) was defined according to the American Psychiatric Association [56] as ‘intellectual and adaptive functioning deficits in conceptual, social, and practical domains’ (p. 37). In general, ID is associated with several characteristics and restrictions in problem solving skills, interpersonal communication, self-care, self-management, etc. The participants in the ID group had a mean age of 26.54 years old (+ 7.78) and attended daily centers in Cyprus (n = 32), France (n = 30), Greece (n = 82) and Portugal (n = 24). The centers provided daily support for the rehabilitation, treatment and enhancement of functionality for the individuals receiving their respective services. The individuals attending these centers were all diagnosed with ID, without comorbid conditions, did not attend any other organized exercise/ physical activity program (e.g. Special Olympics), they were able to follow simple verbal instructions and cues, and were classified according to pre-determined criteria [57,58] to those with either high (n = 61), moderate (n = 69) or low functionality (n = 36). The non-ID group was constituted from 32 undergraduate University students, 25.81 years old (+ 8.73) from Spain.
Measuring instruments
A demographic questionnaire was used initially to gather general information for the participants involved. Accordingly, the following measures were used to assess the health – related physical fitness: anthropometric measures (body height, weight, BMI), sit ups, pushups, long jump, sit and reach, shuttle run and ½ mile (800 meters) walk/ run. The selected measures were selected upon collaboration with the staff involved and constituted parts of the Eurofit special [12] or followed guidelines provided by established measures and scholars in the field [59-61]. Verbal encouragement and support was provided, when necessary, to the individuals in the EG throughout the assessments.
Body height: A ruler or tape measure was placed against the wall. The participants were instructed to remove their shoes, keep arms by their side, feet together and face directly in front. The upper back, buttocks and heels were in contact with the wall. Their height was assessed in centimeters, as the distance from the floor to the highest point of their head.
Body weight: Measured in kgr, at the nearest 0.1 kgr, with an electronic weight measure. The participants were instructed to stand still, with hands by their side, wearing athletic clothes (shorts and t-shirt) and without shoes.
BMI: The participant’s body weight, in relation to their respective height, was estimated with the Body Mass Index (BMI) as follows: Body weight (kgr)/[Body height (m)]2.
Sit ups: The participants performed as many bent knee sit-ups as possible within 30 seconds [59].
Pushups: The participants placed their hands on the floor with the elbows extended, toes (or knees) on the floor and straight back. They performed as many pushups as possible within 30 seconds [60].
Long jump: The participants jumped for distance, from a standing start, and landed with feet together in an upright position [60].
Sit and reach: A sit and reach box was used to assess the flexibility of the hamstrings and low back muscles. The assessment required from the participant’s to sit down, with their feet straight, against the box. The box, in turn, was placed against the wall and the participants were instructed to reach forward, keeping at the same time their legs straight, and place their hands as far in the box as they could. A scale 0-50 cm was placed at the top of the box and the participants had to reach and retain the furthest position for at least two seconds (or a count of two) [59].
Shuttle run: The participants covered the distance between two lines, 15.24 meters apart, pick up a block, and return at the start/finish line with the block at hand, as quickly as they could. A simple hand watch was used for that purpose, and the examiners recorded the time in seconds (e.g. 10 sec 55/100) the participants needed to fulfill the task [60].
The ½ mile (800 meters) walk/run: The participants had to cover the ½ mile (800 meters) distance, walking or running, as quickly as they could. The time required to cover the distance was recorded in minutes and at the nearest second (e.g. 6 minutes and 30 seconds) [61].
Statistical analysis
The Statistical Package for the Social Sciences (SPSS Version 18) was used for data analyses. The data was recorded and checked for outliers, according to the pre specified criteria of + 2 for skewness and + 3.2 for kyrtosis [62,63]. Separate univariate ANOVAs examined the effect of the exercise program in the five European countries, upon the health-related physical fitness of the individuals with and without intellectual disabilities (ID) involved. Intraclass coefficients were used for reliability analyses [64,65]. Specifically, the Intraclass coefficients examined the stability of the assessments across time. Following the criteria of Fleiss [66] and LeBreton and Senter [67], Intraclass coefficients < 0.40 were considered poor, 0.41 to 0.75 fair to good, and > 0.75 were considered excellent. The 0.05 level of significance was selected to test the null hypotheses, with univariate post hoc comparisons and Bonferroni adjustments (0.05/c). The criteria of Cohen, et al. [68], were used to evaluate the ANOVA effect size (small: 0.01, medium: 0.06, large: 0.14).
Procedures
A power analysis was initially conducted to consider the appropriate sample size to detect significant differences. The effect size of Johnson, et al. [36], was used for that purpose (d = 0.87), since it was considered ‘the first to quantitatively assess the efficacy of a fully-inclusive autonomy-supportive climate on physical activity levels’ (p = 0.428) for individuals with and without developmental disabilities. According to Grimm, et al. [69], with an alpha level of 0.05, power of 0.80 and the criteria of Cohen, et al. [68], (large effect size > 0.80), a minimum of 34 participants were required to detect significance [69].
A purposive sampling design was used to recruit the experimental and control groups. The principles in the daily centers were approached initially and invited to participate in the ‘Alive and Kicking’ program. Upon agreement with the principals, the staff (a coach and a psychologist, both with a minimum of five years of experience with ID populations and employed the last two years at the respective daily centers) were informed for the purposes of the study and asked for their active engagement and participation. The participants with ID were invited afterwards, seeking for their agreement to participate and signed the informed consent. Parental involvement was also necessary, and consensus was provided from all parents and caregivers approached.
The control group was recruited from a University in Spain. The staff involved were faculty members from the Psychology and the Physical Education and Sport Science Departments. The staff initially posted a general sign on campus asking their students to participate. The students who expressed their interest were informed for the purposes of the study in a separate session, provided their agreement to participate and signed the informed consent form.
Accordingly, a 6-month preparatory phase was deemed necessary (February to August 2018), to prepare the staff involved (coaches and psychologists) and the participants for the upcoming intervention (September 2018 to June 2019). The staff received, from the members of the research team, a mixture of group and individual training to develop a range of strategies designed to increase their need supportive behaviour. Initially, they were exposed to one, initial two-hour workshop on the principles of self-determination theory and needs supportive coaching (February 2018). The discussions from this workshop led to the production of a bespoke, 36-page manual for developing and integrating needs supportive coaching with an ID population (May 2018). This manual consisted of a range of reflective exercises and coaching tasks designed to develop a) awareness of current coaching practices and b) strategies to promote self-determined motivation in the target population and was based on existing SDT intervention guides [70,71]. In June 2018, each coach was provided with the finalised manual and was able to email the research team with queries and comments about their coaching and to discuss further any specific element. In addition, an on-line forum was created in which coaches could post comments and reflections on their use of the coaching manual to gain feedback and peer-support. A further, on-line webinar was provided to more fully discuss the intervention procedures and to work through specific questions and suggestions from attending coaches and psychologists.
At mid-June, the staff involved had to organize the participants in the exercise groups for the upcoming intervention. The participants, in the daily centers (EG) and the University (CG), were provided with several options for attending exercise programs such as swimming, track and field, football, basketball, hiking and bicycling. Following the participant’s preference, the staff organized teams of 5 – 8 individuals, who were prepared for the upcoming intervention. The participants were organized into teams, during that period (June to August 2018), and received introductory training, once a week, according to the SDT principles (both EG and CG). During the introductory training, they were all exposed to the training of basic skills, expressed their preference for the activities they were willing to participate, organized their weekly team meetings, set up personal and team goals, and developed a sense of cohesiveness and affiliation with the other team members.
In an attempt to quantify the effect of the preparatory phase, the participants in the experimental (EG) and control (CG) conditions responded to the Youth Sport Environment Questionnaire [72] measuring team cohesion (pre-June vs. post-September). The YSEQ incorporates 18 items and responses are provided on a 9-point Likert type format (from strongly disagree: 1 to strongly agree: 9). The 18 items are classified under two subscales named task cohesion (8 items; e.g. “I like the way we work together as a team”) and social cohesion (8 items; e.g. “some of my best friends are on this team”). Eys, et al. [72], added two spurious (negative) items, to support the detection of invalid responses. The mean subscale scores for both task and social cohesion are estimated from their respective items. In the present study, the participants in the CG responded to the 9-point Likert format provided by Eys, et al. [72]. The participants in the EG, in turn, responded in a pictorial 3-point Likert type format, following previous researchers [51,73] and the method introduced at the initial stage of the ‘Alive and Kicking’ project [74]. The 18 YSEQ items were simplified and rewritten, in a 3-point pictorial format based on a ‘happy face’ variation (from 1: ‘not like me’, 2: ‘a little bit like me’, and 3: ‘like me’). The pictorial YSEQ questionnaire was administered to a pilot sample (n = 5) of individuals with ID and no difficulties were recorded during the data collection process (lasting 12-15 min).
Repeated sample t-tests were used to examine the differences between the pre and post assessments of the preparatory phase, in the task and social cohesion. The results were significant for both groups (EG & CG). Specifically, the participants in the EG had significantly higher mean post test scores, comparing to their pre test scores, in the task (t = -4.297, p = 0.000) and social (t = -2.163, p = 0.034) cohesion subscales respectively. Similarly, the participants in the CG had significantly higher mean scores at post testing, compared to pre testing, in the task (t = -2.350, p = 0.031) and social (t = -2.500, p = 0.023) cohesion subscales as well.
Accordingly, the intervention program was initiated on September 2018 and terminated on June 2019. During that period, each organized team attended the exercise program twice a week, at the end of the daily schedule - usually in the afternoon - while each training session lasted approximately 60-90 minutes. The sessions were cancelled only for the Christmas holidays, from late December to early January (approximately for 3 weeks). The participants attended at least 80% of the training sessions [75] and their data was retained for statistical analysis.
Each training session, for the participants in the EG, was organized in a routine, according to the location of the daily centres and the distance from the facilities where the exercise program was held. The teams were gathering at the end of the day in their respective centre, the equipment was checked, and the participants were entering the buses used for their transportation. One or two extra staff members were usually escorting the team, including a medical staff carrying first aid equipment for the treatment of injuries.
The coaches, in collaboration with the psychologists, were responsible for the training sessions. They observed the training, provided their district guidance and kept a brief diary throughout. The planning was based on the guidelines provided in the preparatory phase and from scholars [36,39] who reported that the autonomy – supportive environments, based on mastery and collaboration, may enhance the physical activity levels of the individuals with ID involved. At the end of each session, the teams gathered their equipment and returned to the bus. A brief discussion was held into the bus, with respect to individual and team goals, affiliation among the team members, and the planning of the next training sessions. The participants were challenged to offer ideas and innovative thoughts for the next sessions, exercises they may like to modify or try, ways to support their interrelatedness as team members, etc.
In turn, the participants from the CG met on campus, where the respective exercise programs were held (swimming, track and field, football, basketball, hiking and bicycling), at the end of classes. The attempt was to follow the same principles and methods followed for the EG. A routine was organized, and the coach was responsible for the planning (in collaboration with the psychologist) and implementation of the training sessions. The participants were offered with alternatives for executing the exercises, in an autonomy – supportive environment, for setting up their individual and group goals, and for strengthening their relationships with the other team members throughout the activities involved. The psychologist was present to help keeping the training diary, observed the training, discussed with the coach and the participants and provided individual or group consultation when necessary.
The assessment of the health-related physical fitness components was planned at the begin (pre-September), during (intermediate-February) and at the end of the intervention program (post-June), during a training session. The coaches were responsible for the data collection process, and the psychologists were present to assist them. The EG provided data from the three repeated assessments (pre-September vs. intermediate-February vs. post-June), while the CG provided data from the pre and post assessments (pre-September vs. post-June). Throughout the preparatory phase and the intervention programme, the members of the research team were available for one-to-one support with the staff involved to discuss the process of using the intervention materials, provide suggestions and guidance.
The skewness and kyrtosis indexes were not above their respective cut off scores (+ 2 for skewness and + 3.2 for kyrtosis) and the dependent variables (body height, weight, BMI, sit ups, pushups, long jump, sit and reach, shuttle run, ½ mile walk/run) were retained for subsequent statistical analyses. The effect of the intervention was examined with repeated ANOVAs, separate across the two groups (EG and CG). The reason was the fact that the EG was assessed three times across the intervention (pre, intermediate and post), while the CG was assessed twice (pre and post). Further, the participants in the CG did not fulfill both the pre and post assessments in the sit and reach and ½ mile walk/run tests. The repeated assessments, separate for the two groups, are presented in table 1.
| Table 1: Pre, Intermediate and Post tests. | |||
| Variable | Pre | Intermediate | Post |
| EG | |||
| Weight | 72.11 + 19.27 | 64.79 + 18.16 | 71.75 + 18.55 |
| Height | 1.65 + .97 | 1.66 + .98 | 1.66 + .97 |
| BMI | 26.39 + 6.19 | 23.49 + 4.86 | 26.28 + 5.87 |
| Sit & Reach | 8.28 + 13.59 | 15.83 + 6.24 | 10.00 + 12.92 |
| Sit Ups | 14.76 + 7.42 | 18.46 + 5.73 | 16.60 + 8.06 |
| Push Ups | 8.10 + 7.76 | 12.08 + 10.01 | 9.46 + 7.57 |
| Long Jump | 92.01 + 49.68 | 143.74 + 47.79 | 96.22 + 48.40 |
| Shuttle Run | 10.44 + 4.46 | 9.85 + 1.45 | 10.18 + 2.81 |
| ½ Mile Walk/ Run | 411 + 159 | 290 + 72 | 374 + 139 |
| EG | |||
| Weight | 70.73 + 12.96 | - | 71.03 + 12.48 |
| Height | 1.68 + .09 | - | 1.68 + .09 |
| BMI | 25.09 + 3.89 | - | 25.11 + 4.36 |
| Sit & Reach | 24.89 + 7.16 | - | - |
| Sit Ups | 15.60 + 5.15 | - | 19.63 + 8.46 |
| Push Ups | 13.52 + 8.43 | - | 16.39 + 7.18 |
| Long Jump | 162.03 + 35.89 | - | 170.79 + 36.49 |
| Shuttle Run | 7.03 + .56 | - | 7.08 + .49 |
| ½ Mile Walk/Run | - | 259.13 + 67.82 | |
Reliability analysis
The Intraclass coefficients were at the appropriate range for both groups. The results are presented in table 2.
| Table 2: Intraclass Reliability Coefficients | ||
| Variable | Intraclass Coefficients | |
| EG | CG | |
| Weight | 0.998 | 0.989 |
| Height | 0.998 | 0.999 |
| BMI | 0.995 | 0.989 |
| Sit & Reach | 0.848 | - |
| Sit Ups | 0.871 | 0.736 |
| Push Ups | 0.976 | 0.941 |
| Long Jump | 0.992 | 0.975 |
| Shuttle Run | 0.953 | 0.978 |
| ½ Mile Walk/Run | 0.942 | - |
Experimental group
The repeated ANOVAs were not significant for the anthropometric measures of body weight (F = 1.741, p = 0.191, η2 = 0.073) and BMI (F = 2.867, p = 0.072, η2 = 0.115). Surprisingly, the results were significant for the body height (F = 9.561, p = 0.002, η2 = 0.303). The univariate post hoc comparisons with Bonferroni adjustment (0.05/2) were: a) significant for the Intermediate vs. Post (F = 11.733, p = 0.002, η2 = 0.348) comparison and b) not significant for the Pre vs. Intermediate (F = 4.632, p = 0.043, η2 = 0.174) comparison.
With respect to the flexibility assessment (sit & reach), the results were significant (F = 8.373, p = 0.001, η2 = 0.295). The post hoc analyses were: a) not significant for the Pre vs. Intermediate (F = 1.473, p = 0.239, η2 = 0.069) but b) significant for the Intermediate vs. Post (F = 6.054, p = 0.023, η2 = 0.232) comparison.
The results were significant with respect to the sit ups (F = 11.085, p = 0.001, η2 = 0.357), pushups (F = 5.848, p = 0.010, η2 = 0.226) and long jump (F = 11.271, p = 0.001, η2 = 0.360) repeated tests. The significance was evident for the Intermediate vs. Post comparisons across the three assessments (sit ups: F = 16.035, p = 0.001, η2 = 0.445; pushups: F = 5.170, p = 0.034, η2 = 0.205; long jump: F = 10.648, p = 0.004, η2 = 0.347), while no significance was found between the Pre and Intermediate (sit ups: F = 0.047, p = 0.830, η2 = 0.002; pushups: F = 2.667, p = 0.118, η2 = 0.118; long jump: F = 1.482, p = 0.238, η2 = 0.069) assessments.
The ANOVAs were significant for the ½ mile walk/run (F = 5.108, p = 0.011, η2 = 0.196) but not significant for the shuttle run (F = 0.203, p = 0.793, η2 = 0.010). With respect to the ½ mile test, the significance was due to the Pre vs. Intermediate comparison (F = 10.635, p = 0.004, η2 = 0.336). No significant differences were found between the Intermediate vs. Post comparison (F = 1.615, p = 0.218, η2 = 0.071).
Control group
The ANOVAs were not significant for the anthropometric measures of body weight (F = 1.864, p = 0.186, η2 = 0.078), body height (F = 1.303, p = 0.266, η2 = 0.056) and BMI (F = 2.259, p = 0.147, η2 = 0.093). The results were significant with respect to the sit ups (F = 13.461, p = 0.001, η2 = 0.391) and pushups (F = 21.488, p = 0.001, η2 = 0.506), but not significant for the long jump (F = 4.012, p = 0.058, η2 = 0.160) and shuttle run (F = 0.938, p = 0.344, η2 = 0.045) tests.
The significant findings, separate for the EG and CG, are presented in figures 1 to 8.
Figure 1: Body fat (%) by different equations. Different letters show significant differences (p = 0,000) in body fat (% BF) between different equations (LSD test). 1SF: b
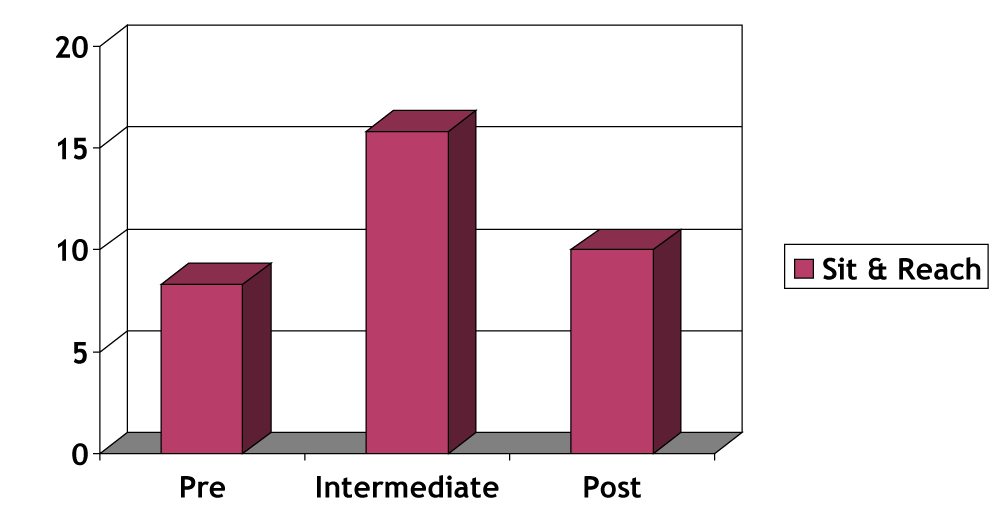
Figure 2: EG: Repeated ANOVAs for the sit and reach (Pre vs. Intermediate: F = 1.473, p = 0.239, η2 = 0.069; Intermediate vs. Post: F = 6.054, p = 0.023, η2 = 0.232).
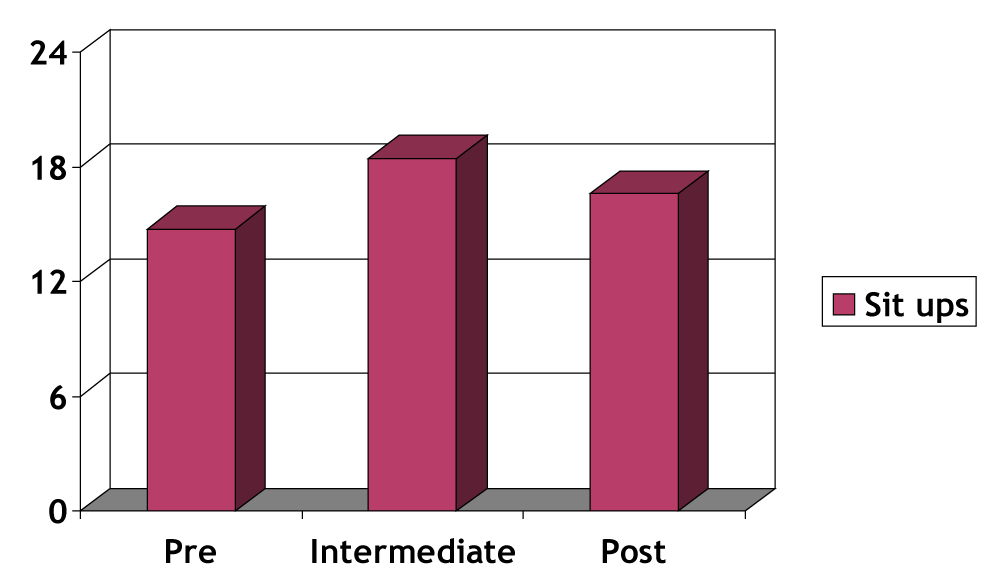
Figure 3: EG: Repeated ANOVAs for the sit ups (Pre vs. Intermediate F = 0.047, p = 0.830, η2 = 0.002; Intermediate vs. Post: F = 16.035, p = 0.001, η2 = 0.445).
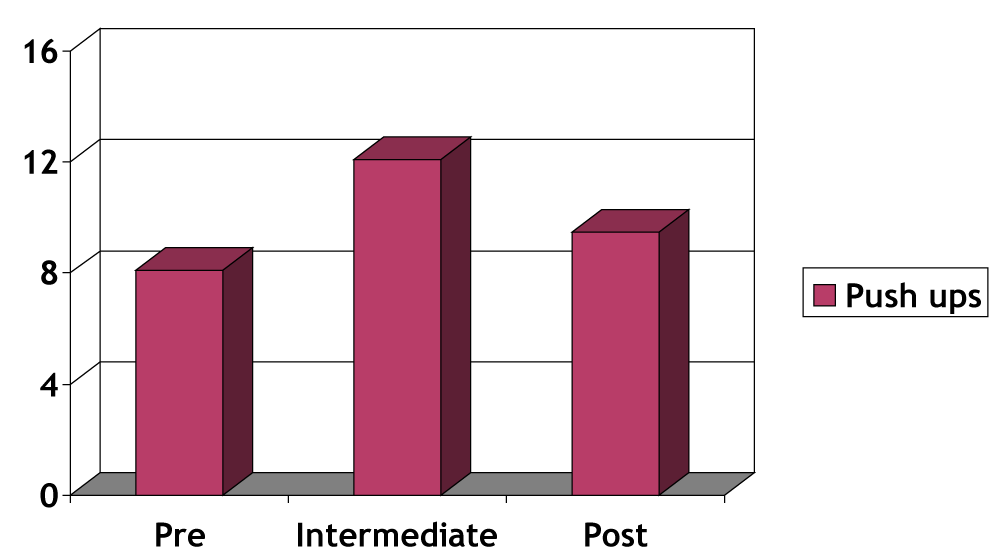
Figure 4: EG: Repeated ANOVAs for the pushups (Pre vs. Intermediate: F = 2.667, p = 0.118, η2 = 0.118; Intermediate vs. Post: F = 5.170, p = 0.034, η2 = 0.205).
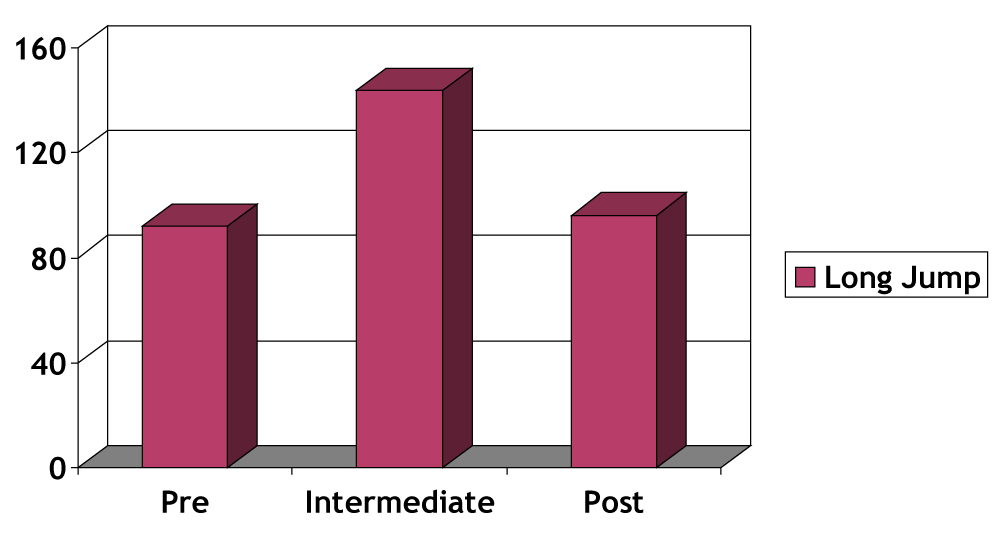
Figure 5: EG: Repeated ANOVAs for the long jump (Pre vs. Intermediate: F = 1.482, p = 0.238, η2 = 0.069; Intermediate vs. Post: F = 10.648, p = 0.004, η2 = 0.347).
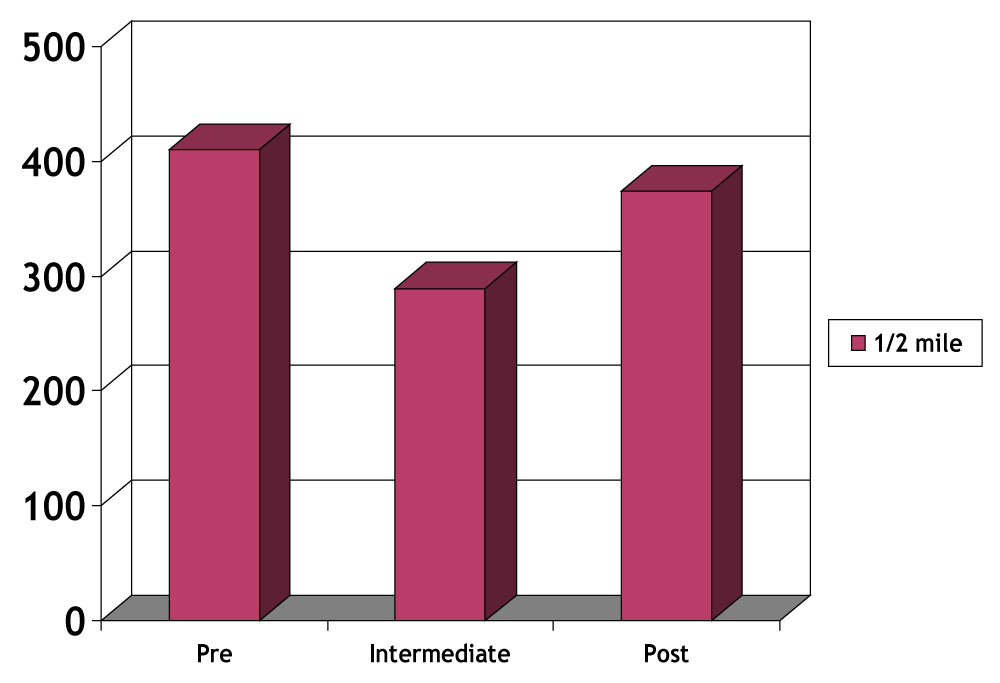
Figure 6: EG: Repeated ANOVAs for the ½ mile walk/ run (Pre vs. Intermediate: F = 10.635, p = 0.004, η2 = 0.336; Intermediate vs. Post: F = 1.615, p = 0.218, η2 = 0.071).
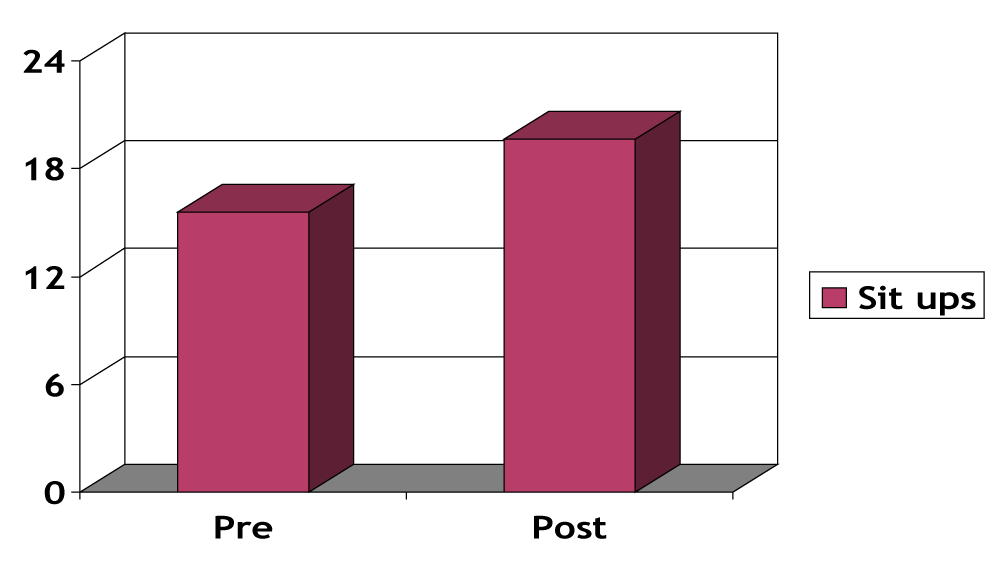
Figure 7: CG: Repeated ANOVAs for the sit ups (F = 13.461, p = 0.001, η2 = 0.391).
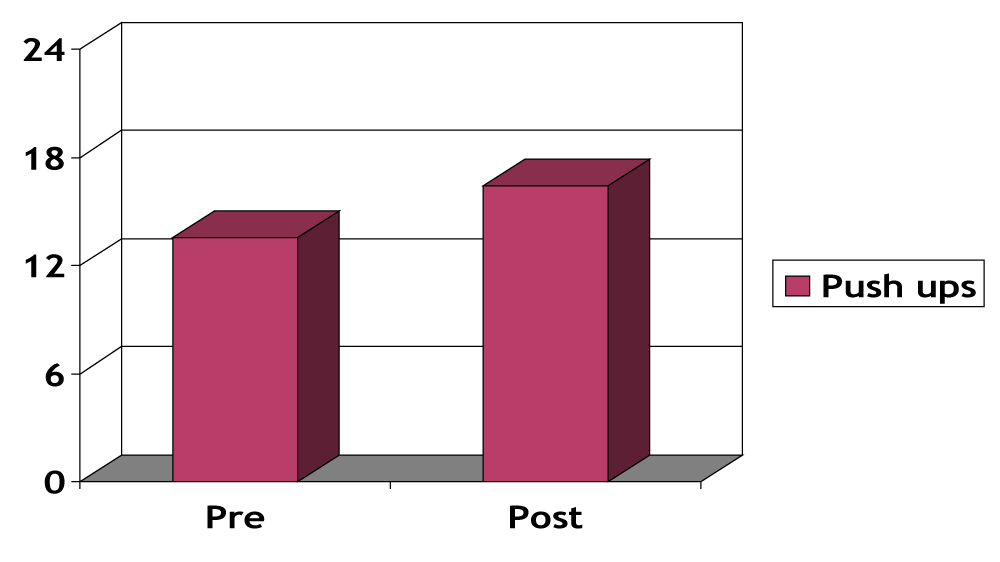
Figure 8: CG: Repeated ANOVAs for the pushups (F = 21.488, p = 0.001, η2 = 0.506).
The study examined the effect of the European-Based ‘Alive and Kicking’ exercise program upon the health-related physical fitness of the individuals with and without intellectual disabilities (ID) involved. The principles of the self-determination theory (SDT) guided the 6-month preparatory phase and the 9-month intervention period throughout. The participants in the experimental group (EG) were recruited from daily centers for individuals with ID, in four European countries (Cyprus, France, Greece and Portugal), while the participants in the control group (CG) were same-aged undergraduate students from Spain. The analyses revealed positive results with respect to the health-related fitness of the ID group who improved their performance, from pre to post testing, in most of the variables assessed (sit & reach, pushups, sit ups, long jump, ½ mile walk/run). The improvement was quicker for the ½ mile aerobic test, from the pre (September) vs. the intermediate (February) assessments. With respect to flexibility (sit & reach), explosive strength (long jump) and muscular endurance (sit ups, pushups), the improvement was attributed to the difference between the intermediate (February) vs. post (June) assessments. In turn, the participants from the CG improved mainly in the muscular endurance components (sit ups and pushups), from the pre (September) to post (June) assessments.
The 9-month intervention was designed to enhance the satisfaction of the basic psychological SDT needs (autonomy, competence, relatedness) and the attainment of intrinsic motivation during the involvement in the exercise program. The enhancement of self-determination was manipulated through the choices provided to the participants during training, the attainment of flexible personal and team goals leading to a climate of excitement, increased persistence, interest and competence, and the sense of belonging to their assigned teams [19,35]. The preparatory phase was deemed essential to prepare both the staff (coach and psychologist) and the participants for the upcoming intervention. During that period, the staff involved became theoretically and practically accustomed to the SDT principles leading to intrinsic motivation, while the participants learned to express their preferences, set up their own and team goals and developed bonds with the staff and their respective team members.
The present findings are in line with the limited number of studies in the field. Carmeli, et al. [76], for example examined a sample of adults with ID who participated in a 10-month exercise intervention study. The researchers reported improvement of their well-being, social acceptance and a high exercise adherence rate of 91.5% for the individuals involved [76]. Simpson, et al. [38], conducted a 12-session intervention, based on the SDT, upon the exercise skills and fitness of individuals with disabilities (including ID). The researcher found that the participants managed to attain their fitness goals, and increased their skills throughout the intervention [38]. Johnson, et al. [36], examined the effect of autonomy based instruction in an inclusive adapted program, on involvement in moderate to vigorous physical activity (MVPA) of individuals with and without developmental disabilities. The researchers stated that the participants spent more time in MVPA during the autonomy based instruction and ‘future studies should consider longer intervention durations, follow-up, or both, to examine the relationship between levels of autonomous climates and physical activity over the long-term’ [36]. Kelly, et al. [35], examined the effect of a six – week yoga intervention program upon the self-determination and anxiety of individuals with developmental and intellectual disabilities. The researcher concluded that the participation was associated with increased self-determination and decreased anxiety for the individuals involved [35]. Kraiss, et al. [37], examined the effect of interventions incorporating a wearable technology (Fitbit) to enhance the involvement in PA of young individuals with intellectual and developmental disabilities. The researcher followed the SDT principles and found that the participants managed to increase their involvement in PA (number of daily steps), reach their personal goals and exhibit consistency in step counts across time [37]. Finally, Hutzler and Korsensky, et al. [39], in a systematic review, examined the motivation correlates towards physical activity (PA) of individuals with ID. The researchers provided the evidence from studies assessing the motivational effects upon, for example, swimming performance and aerobic fitness and concluded that practitioners are not aware of strategies enhancing motivation to support exercise and PA interventions. Possibly, the improvement in physical conditioning during PA and exercise programs may act as a mediator for the enhancement of the psychological determinants and the initiation and maintenance of PA and exercise habits. ‘Further investigations are required to better establish the evidence of effective motivational modalities in facilitating participation in exercise of both young and adult persons with ID’ [39].
The present study is also in line with previous findings examining the association between the involvement in PA/ exercise programs and the SDT elements for individuals with disabilities in general [77-82]. Majnemer, et al. [77], found that individuals with cerebral palsy are benefited in exercise programs that take into consideration their preferences and that seek to enhance their intrinsic motivation. Kwan, et al. [78], reported a direct association between motivation and PA involvement in children with developmental coordination disorder. Sit, et al. [83], found greater involvement in PA during recess (more autonomous) compared to PE instruction (less autonomous) in a sample of children with ID. McLoughlin, et al. [79], attributed the involvement in sports participation to the self-determination motives for athletes with physical disabilities and noted that specific barriers (e.g. cost, time constraints, opportunities) need to be addressed. Perreault, et al. [80], suggested that wheelchair basketball athletes do not differ to their counterparts without disabilities and the exhibited self-determined motivation was associated with elevated involvement and psychological functioning. Banack, et al. [81], reported a strong association between the intrinsic motivation and the perceived coaches’ autonomy and suggested that the athlete’s motivation to compete in Paralympic sports is associated with coaching behavior across time [81]. Finally, Todd, et al. [82], found that an intervention based on the SDT principles enhanced sustained participation in physical activity (cycling) in a group of three individuals with severe autism.
The present findings are promising, and the above literature came up to confirm that argument. But what was happening throughout the 9-month intervention in the five European countries is only something to speculate upon, based on the feedback the research team received from the staff and the examination of their respective diaries. The training sessions were developed by the staff involved and designed to enhance the self-determination elements of autonomy, competence, and relatedness. It can be assumed that the participants always had the option to select the activities they were involved during each session. The coaches introduced the activity stations and the participants were asked to visit the station they preferred, with the other team members, for as long as they desired. These options possibly developed an autonomy-supportive climate which, in turn, led the participants to experience a sense of control [35], increase their active time and engagement in high intensity activities during training [36].
The sequence of the activities and the difficulties the participants faced were progressive, more and more challenging across time and throughout the intervention. The freedom of options in each training session may have increased their excitement and interest, which, in turn, led to higher persistence [19,84]. The participants set up their own goals and worked according to their own potential, under the coaches’ guidance and encouragement, without experiencing negative feedback, comments and threats. This speculation is strengthened from previous researchers who supported a strong association between autonomy and motor competence [85]. Others have reported that the autonomy environment increases the intrinsic motivation, perceptions of ability [86-89] and enhances the achievement of desired outcomes [57]. Further, a direct association between the involvement in PA and the perceived competence of the individuals involved was suggested by Teixeira, et al. [90], while Heller, et al. [91], stated that exercise and health education may enhance the self-efficacy of the individuals involved. According to Deci and Ryan [18], the events enhancing competence may lead to intrinsic motivation, especially when the individual operates in an autonomy structured environment which promotes challenges, positive feedback and ‘freedom from demeaning evaluations’ (p. 70). The present findings are mainly in agreement with the above researchers since the participants stated several times that they managed to reach their personal goals, felt better for themselves, their teammates and coaches across time and improved their skills and fitness levels.
Social bonds were encouraged in the present study, with the other team members, and the staff claimed that the participants developed a sense of belongingness with their teams throughout the preparatory phase and the intervention program. The participants reported that their affiliation with their teammates and the staff was essential for experiencing fun and remain active throughout their involvement. They often encouraged both the staff and their teammates during the training sessions, hugged them and appraised their efforts. Smiles, laughter and positive feedback were the most frequent responses observed and the participants looked forward to the next session. This finding is not in agreement with Edmunds, et al. [92], who stated that the relatedness element of the SDT is frequently under-emphasized in the literature. Frielink, et al. [57], on the other hand claimed that interventions promoting intrinsic motivation are enhanced by feelings of relatedness among team members. Ryan, et al. [93], reported that relatedness is essential in younger individuals, while Pan and Frey [94], claimed that adults and those with developmental disabilities may need additional social support to attenuate changes in their daily exercise habits. According to Johnson, et al. [36], adolescents and adults, with and without disabilities, may require more external support to sustain their motivation and engagement in PA and organized exercise on their own. The external support in the present study was provided by the staff involved in the ‘Alive and Kicking’ program who attempted to enhance the affiliation among the team members, throughout the preparatory and main phases, removed the barriers, retained the interest, and enhanced the intrinsic motivation of the individuals involved throughout the 9-month intervention.
The present study suggests that the intervention study, conducted across five European countries, can improve the health-related physical fitness of the individuals with and without ID involved. This finding is essential if we consider that individuals with ID engage in less than the recommended amount of daily PA [11], experience sedentary lifestyle [1] and elevated risks from associated health problems [6,7]. According to Kraiss, [37], the practitioners need to motivate individuals with and without ID to increase their engagement in PA and exercise programs. This claim is supported by Reid, et al. [95], who stated that individuals with ID often experience low motivation to engage in healthy activities and poor quality of life. The SDT used in the present study provided the general motivation framework that guided the intervention throughout. The findings confirmed previous researchers who stated that self-determination is a significant predictor of health outcomes for individuals with ID [96,97], while others stated that engagement in PA may improve self-determination for individuals with ID [90,98]. In any case, the association between self-determination and engagement in beneficial daily exercise is supported in the present study, but whether engagement in exercise and PA leads to increased self-determination or vice versa is an issue for future researchers to examine.
Certain limitations do not allow generalization of the present findings without caution. First, the ID (experimental) sample was heterogeneous with respect to their country of origin, age and functionality, while the non-ID (control) sample was more homogeneous and constituted from University students who actively participated in the program. Deci, et al. [23], however stated that the ‘psychological nutriments’ of the SDT (autonomy, competence, relatedness) are universal and the culture or location do not alter the requirement to experience satisfaction of the three needs in order to reach intrinsic motivation. The absence of non-participant controls (with and without ID) is in agreement with Hutzler, et al. [39], who claimed, in their systematic review, that only two studies were identified assessing the effect of exercise programs on participants (with ID) vs. non participants. Further, the effect of the intervention upon individuals who differ according to age and functionality is always an option for future researchers to consider. Second, there was no access to personal records and certain conditions, mainly due to confidential policies throughout the five European countries involved. Related syndromes therefore (Down syndrome) or comorbidities, especially for the low functioning ID group, were not recorded [4]. Third, the data collection process during the intervention was conducted from the coaches in general, and the staff involved were present to assist. The coaches were trained and experienced for conducting the assessments, and the reliability evidence confirmed that the data files were proper for statistical analyses. However, specially designed equipment (e.g. motion sensors) were not used [11] and it is uncertain whether the ID group (especially the low functioning) fully attended the tasks, understood exactly what was expected for them to do and gave their best effort throughout [99].
Fourth, both the assessments and the implementation of the ‘Alive and Kicking’ exercise program were conducted from the same individuals, who were not blind to the purposes of the intervention, had previous experience with the individuals involved (both with and without ID), were qualified, trained, and were kept motivated throughout the intervention. This limitation, although necessary to report, is in agreement with Frey, et al. [100], who claimed that lack of staff motivation may be a hazard for effective interventions with individuals with ID. Overall, the effect of social desirability may not be surpassed and future researchers may need to address this issue. Fifth, certain outcome variables may be missing, such as quality of life, depression and anxiety [101]. Sixth, it is uncertain whether the improvement in health-related physical fitness facilitated the participants to become more intrinsically motivated, or whether the intrinsic motivation and the satisfaction of their basic psychological needs (autonomy, competence, and relatedness) led them to engage more actively in the program and improve their health-related physical fitness scores. Seventh, it was not feasible to combine the data files from the ID and non-ID groups, mainly because the IDs were assessed three times throughout the intervention (pre, intermediate, post) while the non-IDs were assessed twice (pre and post). Further, the aerobic fitness improved quicker (from pre vs. intermediate assessments), while flexibility, explosive strength and muscular endurance required a little more time (intermediate vs. post assessments) for the ID group. A solid scientific explanation was not feasible, and the coaching diaries led us to consider that the experimental unit received more aerobic stimuli at the initial stage of the intervention (September through February), while the second stage (February to June) incorporated more stimuli related to the enhancement of flexibility and strength. Still, the significant findings for height were unexpected, but examination of the respective mean scores revealed only minor differences across time for the ID group. The wide sample size therefore may have been the reason for this unexpected finding. Eighth, the present study assimilated a quasi-experimental design, without initial randomization, with an attempt to collect quantitative evidence and generalize the respective findings. A portion of the data however was qualitative and was based upon the coaches’ diaries, anecdotal reports and notes, and the feedback the staff provided to the members of the research team. Future researchers therefore may need to incorporate both quantitative and qualitative methods of data collection (multi-method), with solid methodological procedures to analyze the qualitative evidence (e.g. direct content analysis) in order to support their respective findings [35,102].
Despite these stated limitations, many of them unavoidable given the large-scale, real-world nature of the research design, the current research does provide some promising preliminary evidence to support the feasibility and potential fitness benefits of integrating theoretically informed strategies aimed to enhance motivation into traditional coaching programs for individuals with intellectual disabilities. With a relatively resource-efficient intervention designed to educate coaches how to promote a needs-supportive sporting environment, the present research was able to demonstrate significant improvements in a wide range of physical parameters that are, in turn, predictive of physical and psychological well-being in individuals with ID and contribute to enhanced levels of functioning and integration.
- Rimmer JH, Braddock D. Health promotion for people with physical, cognitive, and sensory disabilities: An emerging national priority. Am J Health Promot. 2002; 16: 220–224. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/11913327
- Frey GC, Stanish HI, Temple VA. Physical activity of youth with intellectual disability: Review and research agenda. Adapt Phy Activ Q. 2008; 25: 95-117. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/18493087
- Hoge G, Dattilo J. Recreation participation patterns of adults with and without mental retardation. Education and Training in Mental Retardation and Developmental Disabilities. 1995; 30: 283-298.
- Temple VA, Frey GC, Stanish HI. Physical activity of adults with mental retardation: Review and research agenda. Am J Health Promot. 2006; 21: 2–12.
- Sutherland G, Couch MA, Iacono T. Health issues for adults with developmental disability. Res Dev Disabil. 2002; 23: 422–445. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/12426010
- Rimmer JH, Braddock D, Fujiura G. Prevalence of obesity in adults with mental retardation: Implications for health promotion and disease prevention. Ment Retard. 1993; 31: 105–110. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/8479328
- Rimmer JH, Braddock D, Marks B. Health characteristics and behaviors of adults with mental retardation residing in three living arrangements. Res Dev Disabil. 1995; 16: 489–499. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/8584768
- Draheim CC, Williams DP, McCubbin JA. Prevalence of physical inactivity and recommended physical activity in community-based adults with mental retardation. Ment Retard. 2002; 40: 436–444. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/12408746
- Graham A, Reid G. Physical fitness of adults with an intellectual disability: A 13-year follow-up study. Res Q Exerc Sport. 2000; 71: 152–161. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/10925812
- Fernhall B, Pitetti KH. Limitations to physical work capacity in individuals with mental retardation. Clinical Exercise Physiology. 2001; 3: 176–185.
- Stanish H, Temple V, Frey G. Health-promoting physical activity of adults with mental retardation. Ment Retard Dev Disabil Res Rev. 2006; 12: 13-21. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/16435324
- Skowronski W, Horvat M, Nocera J, Roswal G, Croce R. Eurofit Special: European fitness battery score variation among individuals with intellectual disabilities. Adapt Phys Activ Q. 2009; 26: 54-67. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/19246773
- Walsh P, Kerr M, Van Schrojenstein L. Health indicators for people with intellectual disabilities. Eur J Public Health. 2003; 13: 47-50. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/14533748
- U.S. Public Health Service. U.S. Surveillance of Health of People with Intellectual Disabilities. 2002.
- Stancliffe RJ, Keane S. Outcomes and costs of community living: A matched comparison of group homes and semi-independent living. J Intellectual and Developmental Disabilities. 2000; 25: 281–305.
- Polder J, Meerding W, Bonneaux L, van der Maas PJ. Healthcare costs of intellectual disability in the Netherlands: A cost-of-illness perspective. J Intellect Disabil Res. 2002; 46: 168–178. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/11869388
- Stancliffe RJ. Living with support in the community: Predictors of choice and self determination. Ment Retard Dev Disabil Res Rev. 2001; 7: 91–98. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/11389563
- Deci EL, Ryan RM. The ‘‘what’’ and ‘‘why’’ of goal pursuits: Human needs and the self-determination of behavior. Psychological Inquiry. 2000; 11: 227–268.
- Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and wellbeing. American Psychologist. 2000; 55: 68–78.
- Ryan RM, Deci EL. Active Human Nature: Self-Determination Theory and the Promotion, and Maintenance of Sport, Exercise and Health. In M.S. Hagger & N.L.D. Chatzisarantis (Eds.), Intrinsic motivation and self-determination in sport and exercise (pp. 1–22). Champaign, IL: Human Kinetics. 2007.
- Deci EL, Ryan RM. Motivation, Personality, and Development within Embedded Social Contexts: An Overview of Self Determination Theory. In R. M. Ryan (Ed.), The Oxford handbook of human motivation (pp. 85–107). Oxford, United Kingdom: Oxford University Press. 2012.
- Deci EL. Promoting intrinsic motivation and self-determination in people with mental retardation. Int Review Res Ment Retardation. 2004; 28: 1–29.
- Deci EL, Ryan RM. Self-determination theory: A macrotheory of human motivation, development, and health. Canadian Psychology. 2008; 49: 182–185.
- Farrell R, Crocker P, McDonough M, Sedgwick W. The driving force: Motivation in Special Olympians. Adapted Physical Activity Quarterly. 2004; 21: 153-166.
- Pannekoek L, Piek J, Hagger M. The Children’s Perceived Locus of Causality Scale for physical education. Journal of Teaching in Physical Education. 2014; 33: 162-185.
- Deci EL, Ryan RM. Intrinsic Motivation and Self-determination in Human Behavior. New York: Plenum Press. 1985.
- Keeney J, Schneider K, Moller A. Lessons learned during formative phase development of an asynchronous, active video game intervention: Making sedentary fantasy sports active. Psychology of Sport & Exercise. 2019; 41: 200-210.
- Rhodes R, Beauchamp M, Blanchard C, Bredin S, Warburton D, et al. Predictors of stationary cycling exergame use among inactive children in the family home. Psychology of Sport & Exercise. 2019; 41: 181-190.
- Johnston C, Davis W. Motivating exercise through social media: Is a picture always worth a thousand words? Psychology of Sport & Exercise. 2019; 41: 119-126.
- Dean D, Griffith D, McKissic S, Cornish E, Johnson-Lawrence V. Men on the move–Nashville: Feasibility and acceptability of a technology enhanced physical activity pilot intervention for overweight and obese middle and older age African American men. Am J Mens Health. 2018; 12: 798–811. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27099346
- Sundar T, Løndal K, Lagerløv P, Glavin K, Helseth S. Overweight adolescents’ views on physical activity – experiences of participants in an internet-based intervention: a qualitative study. BMC Public Health. 2018; 18: 448-456. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/29618327
- Coleman S, Sebire S. Do people’s goals for mass participation sporting events matter? A self-determination theory perspective. J Public Health. 2016; 39: 202–208. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27679656
- Bodde AE, Seo DC, Frey GC, Van Puymbroeck M, Lohrmann DK. The effect of a designed based intervention on physical activity knowledge and participation of adults with intellectual disabilities. Am J Health Promot. 2012; 26: 313-316. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/22548427
- Di Lorito C, Pollock K, Harwood R, das Nair R, Logan P, et al. Protocol for the process evaluation of the promoting activity, independence and stability in early dementia and mild cognitive impairment (PrAISED 2) randomized controlled trial. Maturitas. 2019; 122: 8-21. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/30797535
- Kelly C. The Impact of an Autonomy – Supported Yoga Intervention on the Self – Determination and Anxiety for Individuals with Intellectual and Developmental Disabilities. Master Thesis. Clemson University, South Carolina, USA. 2019.
- Johnson J, Miedema B, Converse B, Hill D, Buchanan A, et al. Influence of high and low autonomy-supportive climates on physical activity in children with and without developmental disability. Journal of Developmental and Physical Disabilities. 2018; 3: 427-437.
- Kraiss K. Evaluating the Effects of Wearable Technologies to Improve Physical Activity Levels for College Students with Intellectual and Developmental Disabilities. Doctoral Dissertation. University of Tennessee, Knoxville, USA. 2017.
- Simpson K. Exploring Exercise and Youth with a Disability. Doctoral Dissertation. The University of Western Ontario, Ontario, Canada. 2012.
- Hutzler Y, Korsensky O. Motivational correlates of physical activity in persons with an intellectual disability: a systematic literature review. J Intellect Disabil Res. 2010; 54: 767–786. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/20712695
- Wullink M, Widdershoven I, van Schrojenstein Lantman-deValk H, Metsemakers I, et al. Autonomy in relation to health among people with intellectual disability: a literature review. J Intellect Disabil Res. 2009; 53: 816-826. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/19646099
- Vallerand RJ, Reid G. Motivation and Special Populations: Theory, Research, and Implications Regarding Motor Behavior. In G. Reid (Ed.), Problems in movement control. Amsterdam: North-Holland. 1990.
- Wehmeyer ML. Self-Determination and Mental Retardation: Assembling the Puzzle Pieces. In H. N. Switzky (Ed.), Personality and motivational differences in persons with mental retardation. Mahwah: Lawrence Erlbaum. 2001.
- Switzky H. Personality and Motivational Differences in Persons with Mental Retardation. New York, NY: Taylor & Francis. 2001.
- Cohen M. Intrinsic motivation in the special education classroom. J Learn Disabil. 1986; 19: 258-261. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/3711728
- Caouette M, Reid G. Influence of auditory stimulation on the physical work output of adults who are severely retarded. Education and Training in Mental Retardation. 1991; 26: 43-52.
- Vallerand RJ. A Hierarchical Model of Intrinsic and Extrinsic Motivation in Sport and Exercise. In G. Roberts (Ed.), Advances in motivation in sport and exercise. Champaign: Human Kinetics. 2001.
- Bybee J, Zigler E. Outer-directedness in Individuals with and without Mental Retardation. A Review. In E. Zigler & D. Bennett-Gates (Eds.). Personality development in individuals with mental retardation. 1999. 165-205.
- Pozeriene J, Adomaitiene R, Ostaseviciene V, Reklaitiene D, Kragniene I. Sport participation motivation of athletes with intellectual disabilities. Sport. 2008; 70: 69–75.
- Shapiro DR. Participation motives of Special Olympics athletes. Adapted Physical Activity Quarterly. 2003; 20: 150–165.
- Hutzler Y, Oz M, Barak S. Goal perspectives and sport participation motivation of special Olympians and typically developing athletes. Res Dev Disabil. 2013; 34: 2149-2160. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/23643768
- Reid G, Vallerand RJ, Poulin C, Crocker P. The development and validation of the pictorial motivation scale in physical activity. Motivation and Emotion. 2009; 33: 161–172.
- Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985; 100: 126-131. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/3920711
- Malina R. Physical Activity and Health of Youth. Constanta: Ovidius University Annals, Series Physical Education and Sport/Science, Movement and Health. 2010.
- Wikipedia. Physical Fitness. 2019.
- The President’s Council on Physical Fitness and Sports. 2019.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC: American Psychiatric Association. 2013.
- Frielink N, Schuengel C, Embregts-Frielink P. Autonomy support, need satisfaction, and motivation for support among adults with intellectual disability: Testing a self-determination theory model. Am J Intellect Dev Disabil. 2018; 123: 33-49. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/29281319
- ICF: International Classification of Functioning, Disability and Health. 2001.
- Winnick J, Short F. The Brockport Physical Fitness Test Manual: A Health Related Assessment for Youngsters with Disabilities (2nd. ed.). Champaign, IL: Human Kinetics. 1999.
- Bruinincks R, Bruininks B. Bruinincks-Oseretsky Test of Motor Proficiency (2nd ed.). Bloomington, MN: AGS Publishers. 2006.
- Mayorga-Vega D, Bocanerga-Parrilla R, Ornelas M, Viciana J. Criterion-related validity of the distance- and time-based walk/run field tests for estimating cardiorespiratory fitness: A systematic review and meta-analysis. PloS One. 2016; 11: 1-24. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/26987118
- George D, Mallery M. SPSS for Windows Step by Step: A Simple Guide and Reference, 17.0 update (10th ed.). Boston, NA: Pearson. 2010.
- Wilson P, Rogers W, Rodgers W, Wild T. The Psychological Need Satisfaction in Exercise Scale. J Sport and Exercise Psychology. 2006; 28: 231-251.
- Pedhazur E, Pedhazur Schmelkin L. Measurement, Design, and Analysis: An Integrated Approach. Hillsdale, NJ: Lawrence Erlbaum Associates. 1991.
- Hair J, Anderson R, Tatham R, Black W. Multivariate Data Analysis (5th ed.). Upper Saddle River, NJ: Prentice-Hall Inc. 1998.
- Fleiss J. The Design and Analysis of Clinical Experiments. New York, NY: Wiley Inc. 1986.
- LeBreton JM, Senter JL. Answers to 20 questions about interrater reliability and interrater agreement. Organizational Research Methods. 2008; 11: 815–852.
- Cohen J. Statistical Power Analysis for the Behavioral Sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum Associates. 1988.
- Grimm L. Statistical Applications for the Behavioral Sciences. New York, NY: John Wiley & Sons Inc. 1993.
- Jago R, Edwards MJ, Sebire SJ, Cooper AR, Powell JE, et al. Bristol girls dance project (BGDP): protocol for a cluster randomised controlled trial of an after-school dance programme to increase physical activity among 11–12 year old girls. BMC Public Health. 2013; 13: 1003-1005. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/24152257
- Langan E, Toner J, Blake C, Lonsdale C. Testing the effects of a self-determination theory-based intervention with youth Gaelic football coaches on athlete motivation and burnout. Sport Psychologist. 2015; 29: 293-301.
- Eys MA, Lougheed TB, Steven R, Carron AV. Development of a cohesion questionnaire for youth: the youth sport environment questionnaire. J Sport Exerc Psychol. 2009; 31: 390-408. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/19799000
- Zoerink D, Wilson J. The competitive disposition: Views of athletes with mental retardation. Adapted Physical Activity Quarterly. 1995; 12: 34-42.
- Skordilis E, Greenlees I, Chrysagis N, Grammatopoulou E, Papadopoulou V, et al. Validity and reliability evidence of the Basic Psychological Needs in Exercise Scale (BPN-ES) in a European sample of individuals with intellectual disabilities. World Journal of Research and Review. 2019; 8: 6-15.
- Carroll K. Enhancing Retention in Clinical Trials of Psychosocial Treatments: Practical Strategies. NIDA Res Monogr. 1997; 165: 4-24. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/9243544
- Carmeli E, Orbach I, Zinger-Vaknin T, Morad M, Merrick J. Physical training and well-being in older adults with mild intellectual disability: a residential care study. Journal of Applied Research in Intellectual Disability. 2008; 21: 457–465.
- Majnemer A, Shevell M, Law M, Birnbaum R, Chilingaryan G, et al. Participation and enjoyment of leisure activities in school-aged children with cerebral palsy. Dev Med Child Neurol. 2008; 50: 751-758. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/18834388
- Kwan M, Cairney J, Hay J, Faught B. Understanding physical activity and motivations for children with Developmental Coordination Disorder: An investigation using the Theory of Planned Behavior. Res Dev Disabil. 2013; 34: 3691-3698. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/24013157
- McLoughlin G, Weisman Fecske C, Castaneda Y, Gwin C, Graber K. Sport participation for elite athletes with physical disabilities: Motivations, barriers, and facilitators. Adapt Phys Activ Q. 2017; 34: 421–441. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/28985104
- Perreault S, Vallerand R. A test of self determination theory with wheelchair basketball players with and without disability. Adapt Phys Activ Q. 2007; 24: 305–316. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/18042968
- Banack H, Sabiston C, Bloom G. Coach autonomy support, basic need satisfaction, and intrinsic motivation of Paralympic athletes. Res Q Exerc Sport. 2011; 82: 722-730. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/22276414
- Todd Τ, Reid G, Butler-Kisber L. Cycling for students with ASD: Self-regulation promotes sustained physical activity. Adapt Phys Activ Q. 2010; 27: 226-241. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/20571157
- Sit CH, McKenzie TL, Lian JM, McManus A. Activity levels during physical education and recess in two special schools for children with mild intellectual disabilities. Adapt Phys Activ Q. 2008; 25: 247–259. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/18765864
- Deci EL, Ryan RM. The support of autonomy and the control of human behavior. J Pers Soc Psychol. 1987; 53: 1024-1037. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/3320334
- Valentini NC, Rudisill ME. An inclusive mastery climate intervention and the motor skill development of children with and without disabilities. Adapt Phys Activ Q. 2004; 21: 330–347.
- Ames C. Achievement Goals, Motivational Climate, and Motivational Processes. In G. C. Roberts (Ed.), Motivation in sport and exercise (pp. 161–176). Champaign: Human Kinetics Publishers. 1992.
- Ames C, Archer J. Achievement of goals in the classroom: Students’ learning strategies and motivation processes. Journal of Educational Psychology. 1988; 80: 260–267.
- Parish L, Treasure D. Physical activity and situational motivation in physical education: Influence of the motivational climate and perceived ability. Res Q Exerc Sport. 2003; 74: 173-182. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/12848230
- Treasure D, Roberts G. Students’ perceptions of the motivational climate, achievement beliefs, and satisfaction in physical education. Res Q Exerc Sport. 2001; 72: 165–175. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/11393879
- Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: A systematic review. Int J Behav Nutr Phys Act. 2012; 9: 1-30. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/22726453
- Heller T, Hsieh K, Rimmer JH. Attitudinal and psychosocial outcomes of a fitness and health education program on adults with Down Syndrome. Am J Ment Retard. 2004; 109: 175-185. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/15000672
- Edmunds J, Ntoumanis N, Duda JL. Testing a self-determination theory based teaching style intervention in the exercise domain. European Journal of Social Psychology. 2008; 38: 375–388.
- Ryan RM, Grolnick WS. Origins and lawns in the classroom: Self-report and projective assessments of individual differences in children’s perceptions. Journal of Personality and Social Psychology. 1986; 50: 550-558.
- Pan CY, Frey GC. Physical activity patterns in youth with autism spectrum disorders. J Autism Dev Disord. 2006; 36: 597-601. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/16652237
- Reid K, Smiley E, Cooper S. Prevalence and associations of anxiety disorders in adults with intellectual disabilities. J Intellect Disabil Res. 2011; 55: 172–181. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/21205039
- Carraro A, Gobbi E. Effects of an exercise programme on anxiety in adults with intellectual disabilities. Res Dev Disabil. 2012; 33: 1221–1226. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/22502848
- Emond Pelletier J, Joussemet M. The benefits of supporting the autonomy of individuals with mild intellectual disabilities: An experimental study. J Appl Res Intellect Disabil. 2017; 30: 830–846. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27461950
- Martinsen EW. Physical activity in the prevention and treatment of anxiety and depression. Nord J Psychiatry. 2008; 62: 25–29. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/18752115
- Horvat M, Block M, Kelly K. Developmental and Adapted Physical Activity Assessment. Champaign, IL: Human Kinetics. 2007.
- Frey GC, Buchanan AM, Sandt DR. “I’d rather watch TV”: An examination of physical activity in adults with mental retardation. Ment Retard. 2005; 43: 241-254. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/16000025
- Hutzler Y, Sherrill C. Disability, Physical Activity, Psychological Well-being and Empowerment: A Life Span Perspective. In R. Lidor, & M. Bar-Eli (Eds.), Sport psychology: Linking theory and practice (pp. 281-300). Morgantown, WV: Fitness Information Technology. 1999.
- Karkaletsi F, Skordilis E, Evaggelinou C, Grammatopoulou E, Spanaki E. Research trends in adapted physical activity on the base of APAQ journal (2006-2010). European Journal of Adapted Physical Activity. 2012; 5: 45-64.
- Temple VA, Walkley JW. Physical activity of adults with intellectual disability. Journal of Intellectual and Developmental Disabilities. 2003; 28: 323–334.