Research Article
Vertebral pain syndrome and physical performance assessing in older women with vertebral fractures

Grygorieva Nataliia*, Povorozyuk Vladyslav and Rybina Olena
Institute of Gerontology named after D. F. Chebotarev NAMS of Ukraine, Kyiv, Ukraine
*Address for Correspondence: Grygorieva Nataliia, Institute of Gerontology named after D. F. Chebotarev NAMS of Ukraine, Kyiv, Ukraine, Tel: +38(044) 430-41-74, Email: crystal_ng@ukr.net
Dates: Submitted: 06 October 2017; Approved: 16 October 2017; Published: 17 October 2017
How to cite this article: Grygorieva N, Povorozyuk V, Rybina O. Vertebral pain syndrome and physical performance assessing in older women with vertebral fractures. J Sports Med Ther. 2017; 2: 109-117. DOI: 10.29328/journal.jsmt.1001015
Copyright License: © 2017 Grygorieva N, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Vertebral fracture; Osteoporosis; Pain; Physical performance; Women

Summary
The purpose of this study was to assess the peculiarities of vertebral pain syndrome, parameters of physical performance and quality of life indices in women of older age depending on the presence of vertebral fractures (VF). This study was performed with participation of 215 women aged 50-89 years old which were divided into two groups: first one-women without any previous osteoporotic fractures (n=143), second group - patients with VF in thoracic and/or lumbar spine (n=72).
The presence and intensity of pain in the thoracic and lumbar spine were evaluated using the 11-component visual analog scale (VAS), physical performance-with following functional tests: 3-, 4- and 15-meter tests (gait speed), static balance (a side-by-side position, a semi-tandem position and a full-tandem position), 8-feet test and «five timed chair stands» (coordination and strength), hand grip strength (by dynamometer), measurement of arterial pressure (systolic and diastolic), heart and respiratory rates, breath holding, chest excursion (mean and on the inhalation and the exhalation), lateral trunk lean, Schober and Thomayer tests.
It was demonstrated that the intensity of vertebral pain (pain at the time of investigation, the most common level of pain, pain in the best periods of the disease) and some physical performance tests (lateral trunk lean and chest excursion (mean index, during the inhalation and exhalation), hand grip strength, 15-meter gait speed test and five-repetition sit-to-stand test) are significantly worse in women with VF than corresponding parameters in persons without fractures. It should be taken into account during the assessment of physical performance and development of rehabilitation programs for older age women with vertebral fractures.
Introduction
Nowadays, vertebral fractures (VF) are one of the frequent and severe complications of systemic osteoporosis, which lead to severe spine pain, restriction of physical activity, increased disability and mortality [1,2]. Numerous studies have confirmed that VF increase the risk of new vertebral and nonvertebral fractures in postmenopausal women [3,4]. In addition, the risk of future VF is also associated with the number of previous VF and the severity of the vertebral deformities [5,6]. Taking into account the important medical and social consequences of VF and their crucial role in the development of the <
The aim of the study was to assess the peculiarities of vertebral pain syndrome, parameters of physical performance and quality of life indices in women of older age depending on the presence of vertebral fractures.
Material and Methods
We utilized a cross-sectional research design. The study was conducted at the D.F. Chebotarev Institute of Gerontology NAMS Ukraine (Kyiv) and approved by Ethics Committee of the Institute. All patients signed informed consent for participation in the study and conservative treatment of osteoporosis in the institute clinic. We examined 215 women aged 50-89 years old (50-59 years - 37 persons, 60-69 - 55 women, 70-79 - 115 persons, 80-89 - 8 patients). Women were divided into two groups: first one women without any previous osteoporotic fractures (n=143), second group - patients with VF in thoracic and/or lumbar spine (n=72). It was found that examined patients did not differ significantly in parameters of age, age of menarche and menopause, duration of the postmenopausal period. However, patients with VF had significantly lower indices of height, weight and body mass index (BMI). In addition, reliable deterioration of BMD parameters of all examined sites (lumbar spine, femoral neck, radius and total body) was established. Clinical characteristics of patients are presented in table 1. The presence and intensity of thoracic and lumbar pain syndrome were evaluated using 11-component Visual Analog Scale (VAS). We measured pain intensity in scores of 0 to 10 during the last week before the survey. Quality of life was measured by EuroQul-5D questionnaire. All women completed the questionnaires independently after a preliminary explanation by the researcher.
| Table 1: Clinical characteristics of women depending on the presence of vertebral fractures. | ||||
| Index / Group | Without any fractures | With vertebral fractures | t | p |
| Age, years | 68.53±7.94 | 68.16±7.37 | 0.33 | 0.74 |
| Height, m | 1.57±0.06 | 1.55±0.07 | 2.17 | 0.03 |
| Weight, kg | 76.57±14.50 | 69.93±13.17 | 3.26 | 0.001 |
| Body mass index, kg/m2 | 30.76±5.46 | 28.75±4.61 | 2.67 | 0.008 |
| Age of menarche, years | 13.86±1.52 | 13.74±1.62 | 0.52 | 0.61 |
| Age of menopause, years | 48.51±5.18 | 48.65±4.42 | 0.19 | 0.85 |
| Duration of postmenopausal period, years | 20.42±8.16 | 19.77±7.79 | 0.55 | 0.58 |
| BMD of lumbar spine (L1–L4), g/cm2 | 1.06±0.22 | 0.89±0.23 | 5.43 | 0.0000001 |
| BMD of femoral neck, g/cm2 | 0.83±0.14 | 0.72±0.11 | 5.93 | 0.0000001 |
| BMD of total radius, g/cm2 | 0.57±0.10 | 0.49±0.10 | 5.25 | 0.0000001 |
| BMD of total body, g/cm2 | 0.91±0.15 | 0.79±0.13 | 5.86 | 0.0000001 |
| Note: Data presented as mean ± SD. | ||||
Moreover, the research tool consisted of a series of following functional tests.
Gait speed was measured by 3-, 4- and 15-meter tests. Results of these tests were the time which it took patients to walk these distances along a corridor. The best performance achieved in two walks at the participant’s usual pace along a corridor 3-, 4- or 15 meters long was recorded in meters/sec. Participants were allowed to use any additional devices (canes, walkers etc.) [17,18]. Static balance ability was measured by 3 increasingly difficult standing balance tests. Participants were asked to maintain their balance in three different positions (a side-by-side position (SBSP), a semi-tandem position (STP), and a full-tandem position (FTP)). The time taken to complete the test was recorded in seconds [17]. Coordination and strength was measured by «five timed chair stands» test and recorded in seconds. Participants were asked to stand up and sit down five times as quickly as possible, with their hands folded across their chest. Also 8-feet test was measured (patient goes ahead and places one foot in front of the other, heel to toe for 8 feet. The ability to perform this test reflects the patient coordination) [17,18]. In addition, physical examination was performed and included the measure of arterial pressure (systolic and diastolic, mm Hg), heart and respiratory rates (n/sec), breath holding (sec), chest excursion (mean and on the inhalation and the exhalation, lateral trunk lean, cm) and assessment of Schober and Thomayer tests (cm). Chest excursion [19,20] was measured by centimeter on the level of 4th ribs. In addition, thoracic excursion was metered at maximal inhalation and exhalation. Usually the chest circumference difference between the maximal inhalation and exhalation is 6-8 cm. Schober test [21,20] reflects the limitation in the lumbar spine and measures the patient’s ability to flex the lower back. Investigator finds L5 of the lumbar vertebrae, puts a dot, measures upwards 10 cm and makes a second dot. After patient leaning forward without bending the knees the second measure of distance between 2 dots is performed. Decrease of the distance less than 4-5 cm gives the evidence about spine limitation.
Thomayer test [20], evaluates the overall mobility of spine. This test, as a previous one, is done with the patient standing straight. Investigator measures the distance from the end of the 3d finger outstretched arms to the floor with maximum inclination ahead. The normal result is 0 and it increases when bending of a spine is restricted. Hand grip strength was measured by the amount of static force that hand can squeeze around a dynamometer and recorded in kilograms [22]. Bone mineral density of lumbar spine, femoral neck and total radius were measured using the dual-energy X-ray absorptiometry (DXA) method (Prodigy, GE Lunar, Madison, 2005, USA). The statistical analysis was carried out using the methods of descriptive statistics, Student’s t-test for independent variables and one-way analysis of variance (ANOVA), Pearson and Spearman correlations for parametric and nonparametric variances. All parameters are represented at mean (M)±standard deviation (SD). Software’s packages of “Statistica 6.0” Copyright License© StatSoft, Inc. 1984-2001 were used during the analysis.
Results
Analysis of our results showed the significant influence of age on variability of vertebral pain intensity at lumbar spine (for most common level of pain - F=7.97; p=0.00006) and its absence at thoracic spine (F=0.56; p=0.63) in women without any previous fractures. In contrast to these results we did not find any reliable influence of age on parameters of pain intensity at thoracic (for most common level of pain - F=0.37; p=0.77) and lumbar (F=0.94; p=0.42) spine in patients with VF. Assessment of VAS parameters in women depending on the presence of VF showed the reliable differences in some indices of the pain severity at thoracic and lumbar spine (Table 2). Indices of pain at the time of investigation, most common level of pain, pain in the best periods of the disease at thoracic and lumbar spine in patients with VF were significant higher than parameters in women without any previous fractures. Other parameters of VAS did not differ at thoracic and lumbar spine depending on previous VF. In addition, current study showed the significant influence of age on variability of parameters of life quality in patients with VF (F=3.90; p=0.013) and women without any previous fractures (F=10.04; p=0.000005). Moreover, the significant correlation between intensity of thoracic pain at the time of investigation and BMD indices at lumbar spine (r=-0.21, p=0.01), femoral neck (r=-0.21, p=0.01), total body (r=-0.22, p=0.007) and quality of life (r=-0.18, p=0.03) was found, but no parameters of physical performance in women without previous fractures. In patients with VF intensity of thoracic pain at the time of investigation reliably correlated with parameters of lateral chest lean (r=-0.31, p=0.02), breath holding (r=-0.33, p=0.02), heart rate (r=0.30, p=0.03) in the absence of relationship with BMD and quality of life parameters.
| Table 2: Intensity of vertebral pain (according 11component VAS) at thoracic and lumbar spine in women of older age group depending on the presence of vertebral fractures, cm. | ||||||||
| Index / Group | Thoracic spine | Lumbar spine | ||||||
| Without any fractures | With vertebral fractures | t | p | Without any fractures | With vertebral fractures | t | p | |
| Pain at the time of investigation | 1,60±2,35 | 2,42±2,84 | 2,14 | 0,03 | 4,12±2,28 | 4,77±2,07 | 1,95 | 0,05 |
| The most common level of pain | 1,24±1,84 | 2,11±2,59 | 2,73 | 0,007 | 3,42±2,00 | 4,13±1,98 | 2,33 | 0,02 |
| Pain in the best periods of the disease | 0,79±1,26 | 1,29±1,83 | 2,26 | 0,02 | 2,17±1,66 | 2,76±1,76 | 2,30 | 0,02 |
| Pain in the worst periods of the disease | 2,36±3,38 | 3,31±3,74 | 1,78 | 0,08 | 6,11±2,81 | 6,66±2,35 | 1,35 | 0,18 |
| Start pain | 0,99±1,55 | 1,50±2,22 | 1,88 | 0,06 | 2,74±1,89 | 3,21±2,26 | 1,53 | 0,13 |
| Pain during long walking | 1,64±2,49 | 2,34±2,86 | 1,77 | 0,08 | 4,34±2,31 | 4,79±2,18 | 1,30 | 0,19 |
| Pain during long rest (at night) | 0,97±1,58 | 1,21±1,80 | 0,95 | 0,34 | 2,52±2,08 | 2,55±1,89 | 0,09 | 0,93 |
| Permanent (continuous) pain | 1,08±1,73 | 1,45±2,19 | 1,29 | 0,19 | 2,94±2,11 | 3,11±2,11 | 0,55 | 0,58 |
| Pain when walking up the stairs | 1,45±2,31 | 1,87±2,40 | 1,18 | 0,24 | 4,10±2,37 | 4,27±2,07 | 0,49 | 0,63 |
| Pain when walking down the stairs | 1,33±2,15 | 1,81±2,39 | 1,42 | 0,16 | 3,65±2,27 | 3,98±2,16 | 0,97 | 0,33 |
| Pain when walking on a flat surface | 1,34±2,11 | 1,58±2,19 | 0,74 | 0,46 | 3,71±2,22 | 3,84±2,24 | 0,39 | 0,70 |
| Note: Data presented as mean ± SD. | ||||||||
Intensity of lumbar pain at the time of investigation significantly correlates with lateral chest lean (r=-0.21, p=0.01), hand grip strength (r=-0.18, p=0.04) and quality of life (r=-0.22, p=0.008) indices in women without previous fractures. In contrast, in patients with VF we did not find any reliable correlations between severity of lumbar pain at the time of investigation and BMD and physical performance indices, except for correlation with quality of life result (r=0.37, p=0.053). Analysis of the influence of age on physical performance parameters in the patients regarding VF found no significant effect on the variability of Schober, Tomayer tests and chest excursion, blood pressure, respiratory and heart rates regardless of VF. In contrast, according to the one-way Anova analysis, age had a significant impact on the variability of the distance of lateral trunk lean and hand grip strength tests in women without any previous fractures (F=4.87; p=0.003 and F=4.58; p=0.004) in the absent of any influence in patients with vertebral fractures. Similar results were obtained according to the results of 4-meter test (F=3.15, p=0.03 in women without fractures and F=2.42, respectively, p=0.07).
Also, the current study showed significant differences in parameters of lateral trunk lean and chest excursion (mean index, during the inhalation and exhalation) depending on the presence of VF in women aged 50-89 years. All these indices were higher in women without fractures. In contrast, we did not find any significant differences of Schober or Tomayer tests depending on the presence of previous VF. In addition, parameter of hand grip strength test in patients with previous VF was lower than correspondent in women without fractures (accordingly 13, 55±7, 99 vs 16,42±9,39 kg, p=0.03). All other studied indices of physical performance probably did not differ in group depending on the presence of VF (Table 3).
| Таble 3: Indices of physical performance in women of older age group depending on the presence of vertebral fractures, cm. | ||||
| Index / Group | Without any fractures | With vertebral fractures | t | p |
| Tomayer test, cm | 6,76±12,38 | 9,51±15,40 | 1,36 | 0,18 |
| Schober test, cm | 4,19±2,55 | 3,64±2,94 | 1,37 | 0,17 |
| Lateral trunk lean, cm | 14,33±4,80 | 12,05±4,19 | 3,30 | 0,001 |
| Chest excursion, cm | 106,61±11,19 | 102,80±9,41 | 2,39 | 0,02 |
| Chest excursion during the inhalation, cm | 108,92±11,12 | 104,62±9,54 | 2,70 | 0,007 |
| Excursion of the chest on the exhalation, cm | 104,51±11,32 | 101,18±9,47 | 2,07 | 0,04 |
| Respiratory rate (frequency for 1 minute), n | 17,13±2,87 | 17,66±3,08 | 1,21 | 0,23 |
| Breath holding, sec | 21,42±7,70 | 20,14±10,04 | 1,01 | 0,31 |
| Hand grip strength, kg | 16,42±9,39 | 13,55±7,99 | 2,14 | 0,03 |
| Five-repetition sit-to-stand test, sec | 13,37±6,12 | 16,09±8,30 | 2,64 | 0,009 |
| 3-metre gait speed test, m/sec | 9,49±3,43 | 10,17±3,61 | 1,30 | 0,20 |
| 4-metre gait speed test, m/sec | 5,54±2,27 | 5,76±2,08 | -0,68 | 0,50 |
| 15-metre gait speed test, m/sec | 14,63±5,04 | 16,23±5,89 | 2,02 | 0,04 |
| Note. Data presented as mean ± SD.* - significant differences (p<0.01) comparing to women without any previous fractures. | ||||
During the analyses of gait speed parameters, significantly higher indices of 15-meter test in patients with VF in comparison with indices in women without previous fractures were established. However, we did not establish any reliably differences in parameters of 3- or 4-meter tests depending on presence of VF. Moreover, the significant correlations between lumbar spine BMD and mean parameters of chest excursion (r=0.33, p=0.0001), chest excursion during the inhalation (r=0.30, p=0.0005) and chest excursion on the exhalation (r=0.32, p=0.0002) in women without previous fractures were found. Also we established the significant correlations between lumbar spine BMD and mean parameters of chest excursion (r=0.38, p=0.002), chest excursion during the inhalation (r=0.37, p=0.008) and chest excursion on the exhalation (r=0.40, p=0.004) in women with previous VF (Figure 1).
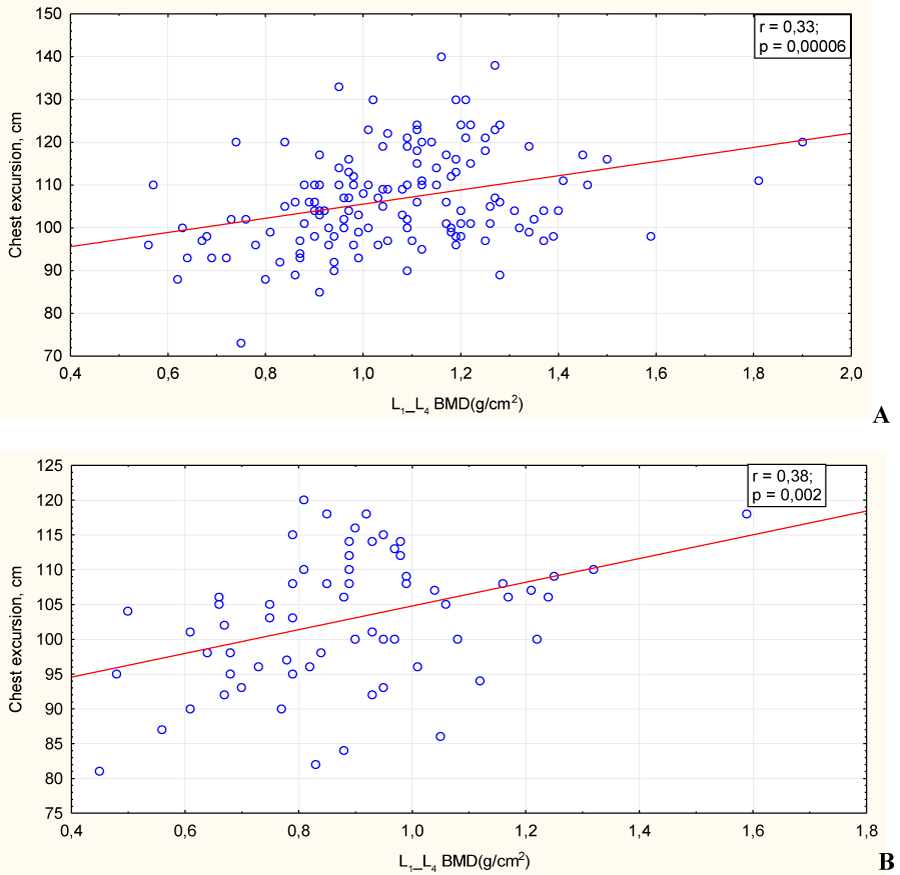
Figure 1: 1A and 1B: Relationship between lumbar spine BMD (L1-L4) and chest excursion in women without (A) and with (B) vertebral fractures. Note: Line represents linear regression of data (A: y = 88.96 + 16.58*x; r2 = 0.11; В: y = 87.75 + 17.0*x; r2 = 0.15).
Indices of quality of life significantly correlated with lateral trunk lean (r=-0.22, p=0.009), hand grip strength (r=-0.20, p=0.02), 4-meter test (r=0.19, p=0.03), 8-feet test (R=-0.19, p=0.03), STP test (R=-0.18, p=0.04), systolic (r=0.23, p=0.006) and diastolic (r=0.20, p=0.006) blood pressure in women without previous fractures. In contrast, we demonstrated the significant correlation only between quality of life indices and results of lateral trunk lean (r=-0.33, p=0.02) and 4-meter test (r=0.32, p=0.02) in women with previous VF. Test of static balance SBSP could not perform 4.8% women without fracture and 3.1% with VF, test in STP - 13.9 and 13.9% women accordingly, test in FTP – 34.0 and 46.2%, 8-feet test - 49.3 and 55.4% women accordingly (p>0.05).
Discussion
Nowadays, VF are serious complications of systemic osteoporosis [1,2,10]. According to the literature, their prevalence in the adult population ranges from 6.2 to 20.7% and depends on the region of residence. Approximately 750 000 new VF are registered in the United States every year among people over 50 years old, and in a quarter of them at least one other vertebral fracture happened during their lifetime. The frequency of VF related to systemic osteoporosis exponentially increases with age. According to WHO data, about 25% of women under 65 already have compression fractures of vertebral bodies. Although VF are often asymptomatic, thoracic or low back pain is one of the most common clinical manifestations of VF.
Vertebral pain in the spine may be associated not only with spine fractures, which is related with systemic osteoporosis, but also with other causes and factors, including different diseases of bone and muscular system (spinal osteochondrosis, scoliosis, etc.), chest, stomach and pelvis, as well as other individual, professional and hormonal risk factors [23]. Thus, Schiphorst Preuper H.R. et al. [24] found that the relative risk of thoracic pain is 5.2 in men (95% confidence interval (CI): 3.9-6.6) and 10.0 (95% CI: 7.8-12.1) in women. The frequency of thoracic pain in men is related to age (odds ratio (OR) – 6.0 (95% CI: 2.1-17.3) in persons 50 years and older), height (OR – 2.2 (95% CI: 1.2-3.9)), frequent static body inclination (OR – 3.0 (95% CI: 1.5-6.1)), lack of recovery periods (OR – 2.0 (95% CI: 1.2-3.6)) and driving of different vehicles (OR – 2.8 (95% CI: 1.4-5.5)). However, it was also found that excessive body weight and obesity are associated with lower risk (OR – 0.5 (95% CI: 0.3-0.96)). In contrast, risk of thoracic pain in women was associated with excessive physical activity (OR – 1.9 (95% CI: 1.1-3.3)) [24].
The results of 52 studies from 65 cohorts found that the frequency of thoracic pain varied within the range of 3.0-55.0%. The individual (female gender, peculiarities of musculoskeletal system development, premenstrual syndrome or postmenopausal), as well as professional (physical labor, high labor intensity, ergonomic problems in the workplace, duration of employment, driving of specialized vehicles) and psychosocial factors (the alleged risk of injury, high psychological stress) increase this risk [23]. Other authors have proved that vertebrate fractures lead not only to the development of pain syndromes, but also to a significant limitation of physical activity [12,14,16].
In addition, the deterioration of the functional capacity is also associated with the number of previous VF and their severity. Thus, it was demonstrated [25] that walking speed in women with two or more compression fractures was significantly slower than that in persons without VF (correspondingly 1.17 and 1.24 m/sec, p=0.03; results were adjusted for age, body mass index, back pain level, number of pain joints, the number of concomitant diseases and level of regular physical activity). Women who had two or more VF had significantly higher (p=0.01) results of the <
According current literature data, low bone mineral density [13,26,27] and increased risk of fall [28,29] are connected with impaired physical performance and both of them increase the risk of future VF. In addition, it was demonstrated early, that, regular exercises are effective non-pharmacological measures in prevention of bone loss and osteoporotic fractures [29-31]. Nowadays, the different tests of physical performance are use for assessment of balancing, coordination, muscle strength and risk of fall in patients with osteoporosis and its complications [14,16,26,28]. Thus, the literature data show that vertebral pain syndrome and associated restriction of physical activity in patients with osteoporosis and its complication (VF) adversely affects the disease progression and life expectancy, as immobilization or low level of physical activity are independent factors of the risk of accelerated bone loss, falls and fractures. The present study sought out to establish the peculiarities of thoracic and lumbar pain, parameters of physical performance and quality of life indices in women of older age depending on the presence of vertebral fractures.
The results of our study showed the significant influence of age on variability of vertebral pain intensity at lumbar spine and its absence at thoracic spine in women without any previous fractures. However, we did not find any reliable influence of age on parameters of pain intensity at thoracic and lumbar spine in patients with VF. These differences may be associated with the development of degenerative changes in the lumbar spine in persons without fractures and their effect on the vertebral pain severity, which requires further study. Moreover, age had a significant impact on the variability of some parameters of physical performance (the distance of lateral trunk lean and hand grip strength) in women without any previous fractures in the absence of any influence on these indices in patients with vertebral fractures. Similar results were obtained according to the results of 4-meter test in women without fractures. Analysis of the influence of age on physical performance parameters in the patients regarding VF found no significant effect on the variability of Schober, Tomayer tests and chest excursion, blood pressure, respiratory and heart rates regardless of VF.
Preliminary studies also indicate deterioration in physical performance tests with age without fractures [18,22,32]. During the study of the parameters of physical performances and risk of fall it was demonstrated that parameters of balancing tests (<
Also, we established the reliable differences in indices of lateral trunk lean and chest excursion (mean index, during the inhalation and exhalation) depending on the presence of VF. All these indices were higher in women without fractures. In contrast, we did not find any significant differences of Schober or Tomayer tests depending on the presence of previous VF. In addition, parameter of hand grip strength in patients with previous VF was lower than corresponding parameters in women without fractures. All other studied indices of physical performance did not differ significantly in group depending on the presence of VF. Our study demonstrated the significant correlations between intensity of thoracic pain at the time of investigation and BMD indices at lumbar spine, femoral neck, total body and quality of life were found, but no parameters of physical performance in women without previous fractures. In patients with VF, intensity of thoracic pain at the time of investigation reliably correlated with parameters of lateral chest lean, breath holding and the heart rate in the absence of relationship with BMD and quality of life parameters.
Intensity of lumbar pain at the time of investigation significantly correlates with lateral chest lean, hand grip strength and quality of life indices in women without previous fractures. In contrast, in patients with VF, we did not find any reliable correlations between severity of lumbar pain at the time of investigation and BMD and physical performance indices, except the correlation with quality of life result. The current study established significantly higher indices of 15-meter test in patients with VF in comparison with parameters of women without previous fractures. However, we did not find any reliable differences in parameters of 3- or 4-meter tests depending on the presence of VF. Moreover, the significant correlations between lumbar spine BMD and mean parameters of chest excursion, chest excursion during the inhalation and chest excursion of the on the exhalation in women without previous fractures were demonstrated. Also we established the significant correlations between lumbar spine BMD and mean parameters of chest excursion, chest excursion during the inhalation and chest excursion of the on the exhalation in women with previous VF.
In our study, indices of quality of life significantly correlated with lateral trunk lean, hand grip strength, 4-meter test, 8-feet test, STP test, systolic and diastolic blood pressure in women without previous fractures. In contrast, we established the significant correlations only between the quality of life indices and results of lateral trunk lean and 4-meter test in women with previous VF.
In conclusion, the intensity of vertebral pain (pain at the time of investigation, the most common level of pain, pain in the best periods of the disease) and some physical performance tests (lateral trunk lean and chest excursion (mean index, during the inhalation and exhalation), hand grip strength, 15-meter gait speed test and five-repetition sit-to-stand test) are significantly worse in women with VF than corresponding parameters in persons without fractures. It should be taken into account in the assessment of physical performance and development of rehabilitation programs for older age women with vertebral fractures.
References
- Griffith JF, Guglielmi G. Vertebral fracture. Radiol Clin North Am. 2010; 48: 519-529. Ref.: https://goo.gl/VeKHhM
- Povorozyuk VV, Grygorieva NV, Orlyk TV et al.Osteoporosis in the practice of an internist-doctor. Expres Кyiv. 2014; 198.
- Black DM, Arden NK, Palermo L, Pearson J, Cummings SR. Prevalent vertebral deformities predict hip fractures and new vertebral deformities but not wrist fractures. Study of Osteoporotic Fractures Research Group. J Bone Miner. Res. 1999; 14: 821-828. Ref.: https://goo.gl/YNCuVJ
- Chen P, Krege JH, Adachi JD, Prior JC, Tenenhouse A, et al. Vertebral Fracture Status and the World Health Organization Risk Factors for predicting osteoporotic fracture risk. J Bone Miner Res. 2009; 24: 495-502. Ref.: https://goo.gl/6AhFHf
- Delmas PD, Genant HK, Crans GG, Stock JL, Wong M, et al. Severity of prevalent vertebral fractures and the risk of subsequent vertebral and nonvertebral fractures: Results from the MORE trial. Bone. 2003; 33: 522-532. Ref.: https://goo.gl/MofiZn
- Pongchaiyakul C, Nguyen ND, Jones G, Center JR, Eisman JA, et al. Asymptomatic vertebral deformity as a major risk factor for subsequent fractures and mortality: A long-term prospective study. J Bone Miner Res. 2005; 20: 1349-1355. Ref.: https://goo.gl/Dz2Hoh
- Camacho PM, Petak SM, Binkley N, Clarke BL, Harris ST, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Clinical Practice Guidelines for the diagnosis and treatment of postmenopausal osteoporosis-2016--Executive Summary. Endocr Pract. 2016; 22: 1111- 1118. Ref.: https://goo.gl/LE2ovF
- Kanis JA, McCloskey EV, Johansson H, et al. On behalf of the Scientific Advisory Board of the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) and the Committee of Scientific Advisors of the International Osteoporosis Foundation (IOF) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2013; 24: 23-57. doi: 10.1007/s00198-012-2074-y.
- Orlyk TV, Grygorieva NV, Povoroznyuk VV. Features of vertebral pain syndromes in older women depending on the duration of postmenopausal period and bone mineral density indices. Adv Gerontol. 2017; 30: 298-305. Ref.: https://goo.gl/9Cnbir
- Cawthon PM, Blackwell TL, Marshall LM, Fink HA, Kado DM, et al. Osteoporotic Fractures in Men (MrOS) Research Group. Physical performance and radiographic and clinical vertebral fractures in older men. J Bone Miner Res. 2014; 29: 2101-2108. Ref.: https://goo.gl/ECzTB3
- Gregg EW, Pereira MA, Caspersen CJ. Physical activity, falls, and fractures among older adults: a review of the epidemiologic evidence. J Am Geriatr Soc. 2000; 48: 883-893. Ref.: https://goo.gl/rQAGHf
- Jinbayashi H, Aoyagi K, Rossetal PD. Prevalence of vertebral deformity and its associations with physical impairment among Japanese women: The Hizen-Oshima Study. Osteoporos Int. 2002; 13: 723-730. Ref.: https://goo.gl/kA5isM
- Logan S, Thu WPP, Lay WK, Wang LY, Cauley JA, et al. Chronic joint pain and handgrip strength correlates with osteoporosis in mid-life women: a Singaporean cohort. Osteoporos Int. 2017. Ref.: https://goo.gl/fDux9x
- Lyles KW, Gold DT, Shipp KM, Pieper CF, Martinez S, et al. Association of osteoporotic vertebral compression fractures with impaired functional status. Am J Med. 1993; 94: 595-601. Ref.: https://goo.gl/ynSyjE
- Stattin K, Michaëlsson K, Larsson SC, Wolk A, Byberg L. Leisure-Time Physical Activity and Risk of Fracture: A Cohort Study of 66,940 Men and Women. J Bone Miner Res. 2017; 32: 1599-1606. Ref.: https://goo.gl/c44X2Z
- Wang LY, Liaw MY, Huang YC, Lau YC, Leong CP, et al. Static and dynamic balance performance in patients with osteoporotic vertebral compression fracture. J Back Musculoskelet Rehabil. 2013; 26: 199-205. Ref.: https://goo.gl/Nsrja6
- Guralnik JM. Assessing physical performance in the older patient [CD-ROM]. Nat Institutes of Aging. 2017.
- Veronese N, Bolzetta F, Toffanello ED, Zambon S, De Rui M, et al. Association Between Short Physical Performance Battery and Falls in Older People: The Progetto Veneto Anziani Study. Rejuvenation Res. 2014; 17: 276-284. Ref.: https://goo.gl/Ca22yQ
- Adedoyin RA, Adeleke OE, Fehintola AO, Gregory EE, Luqman Adeleke B. Reference Values for Chest Expansion among Adult Residents in Ile-Ife. Journal of Yoga & Physical Therapy. 2012; 2: 113. Ref.: https://goo.gl/fD1fYX
- Main symptoms and syndromes in rheumatology. Ref.: https://goo.gl/hDaL3Q
- Buckup K. Clinical Tests for the Musculoskeletal System. Examinations-Signs-Phenomena Thieme Stuttgart New York. 2004. Ref.: https://goo.gl/gAhgsN
- Massy-Westropp NM, Gill TK, Taylor AW, Bohannon RW, Hill CL. Hand Grip Strength: age and gender stratified normative data in a population-based study. BMC Res Notes. 2011; 4: 127. Ref.: https://goo.gl/5UwQoY
- Briggs AM, Smith AJ, Straker LM, Bragge P. Thoracic spine pain in the general population: prevalence, incidence and associated factors in children, adolescents and adults. A systematic review. BMC Musculoskelet Disord. 2009; 29: 10-77. Ref.: https://goo.gl/GSBuQe
- Schiphorst Preuper HR, Reneman MF, Boonstra AM, Dijkstra PU, Versteegen GJ, et al. Relationship between psychological factors and performance-based and self-reported disability in chronic low back pain. Eur Spine J. 2008; 17: 1448-1456. Ref.: https://goo.gl/6inxSh
- Arima K, Abe Y, Nishimura T, Okabe T, Tomita Y, et al. Association of vertebral compression fractures with physical performance measures among community-dwelling Japanese women aged 40 years and older. BMC Musculoskelet Disord. 2017; 18: 176. Ref.: https://goo.gl/bR4m9F
- Singh H, Kim D, Bemben MG, Bemben DA. Relationship between muscle performance and DXA-derived bone parameters in community-dwelling older adults. J Musculoskelet Neuronal Interact. 2017; 17: 50-58. Ref.: https://goo.gl/uvhKzN
- Whitfield GP, Kohrt WM, Pettee Gabriel KK, Rahbar MH, Kohl HW 3rd. Bone mineral density across a range of physical activity volumes: NHANES 2007-2010. Med Sci Sports Exerc. 2015; 47: 326-334. Ref.: https://goo.gl/E57dbd
- Kikkert LHJ, de Groot MH, van Campen JP, Beijnen JH, Hortobágyi T, et al. Gait dynamics to optimize fall risk assessment in geriatric patients admitted to an outpatient diagnostic clinic. PLoS One. 2017; 12: e0178615. Ref.: https://goo.gl/FQwTVY
- Sinaki M. Exercise for patients with osteoporosis: management of vertebral compression fractures and trunk strengthening for fall prevention. PMR. 2012; 4: 882-888. Ref.: https://goo.gl/gZxzSk
- Barry DW, Kohrt WM. Exercise and the preservation of bone health. J Cardiopulm Rehabil Prev. 2008; 28: 153-162. Ref.: https://goo.gl/qz2h4j
- Bolam KA, van Uffelen JG, Taaffe DR. The effect of physical exercise on bone density in middle-aged and older men: a systematic review. Osteoporosis Int. 2013; 24: 2749-2762. Ref.: https://goo.gl/Vvs7VD
- Povoroznyuk VV, Dzerovich NI, Belinska AС, Tkachuk AА. Skeletal muscle tissue state in women of the Ukrainian population. Pain. Joints Spine. 2015; 4: 15-18. Ref.: https://goo.gl/diY5EU
- Wong AY, Karppinen J, Samartzis D. Low back pain in older adults: risk factors, management options and future directions. Scoliosis Spinal Disord. 2017; 18: 12-14. Ref.: https://goo.gl/uHo9Eq